
{kind=link}
| Author | Affiliation |
|---|---|
| Jason Bryant, MD | Kaiser Santa Clara Medical Center, Department of Emergency Medicine, Santa Clara, CA |
| Joel T. Levis, MD, PhD | Kaiser Santa Clara Medical Center, Department of Emergency Medicine, Santa Clara, CA |
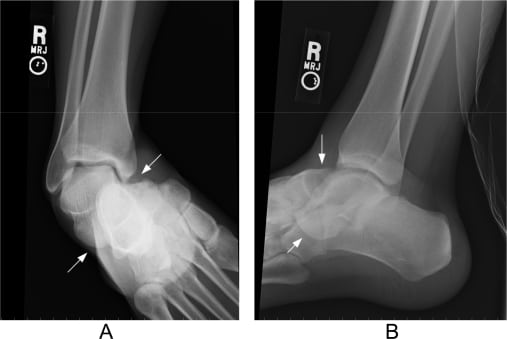
A 26-year-old male presented to the emergency department for right foot pain and deformity after inverting his foot while base running playing baseball. Examination revealed a medial deformity of the right foot (Figure 1). The foot was neurovascularly intact without wounds. Radiographs of the ankle demonstrated a medial subtalar dislocation (Figure 2). The dislocation was reduced using procedural sedation with longitudinal-lateral distraction of the foot, resulting in anatomic reduction of the talocalcaneal and talonavicular joints. The patient was placed in a short leg splint, instructed to remain non-weight-bearing on the right foot, with follow-up in the orthopedic clinic the following day.

Subtalar dislocations are rare injuries accounting for approximately 1% of all dislocations.1 They result from high-energy trauma (e.g., fall from a height or a motor vehicle collision), and certain athletic injuries.1 Inversion of the foot results in a medial subtalar dislocation (80–85% of these injuries), whereas eversion produces a lateral dislocation.2,3 In either case, the talonavicular and talocalcaneal joints are involved simultaneously, while the tibiotalar and calcaneocuboid joints remain intact.3 Optimal management of subtalar dislocations is immediate closed reduction with procedural sedation.1–3 Medial dislocations have a better prognosis compared to lateral, anterior or posterior injuries, which are often associated with fractures, require open reduction and fixation, and frequently result in instability and arthritis.1 A CT scan is sometimes recommended to evaluate for associated osteochondral lesions, although these are uncommon with medial dislocations.1,2 Following reduction, the foot should be immobilized with a short leg cast for 4–6 weeks with the patient remaining non-weight-bearing.3
Footnotes
Supervising Section Editor: Rick A. McPheeters, DO
Submission history: Submitted July 16, 2008; Revision Received August 12, 2008; Accepted August 19, 2008.
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Joel T. Levis, MD, PhD, Department of Emergency Medicine, Kaiser Santa Clara Medical Center 700 Lawrence Expressway, Santa Clara, CA 95051
Email: joellevis@yahoo.com
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Wagner R, Blattert TR, Weckbach A. Talar dislocations. Injury. 2004;35:SB36–SB45.[PubMed]
2. Jerome JTJ, Varghese M, Sankaran B. Anteromedial subtalar dislocation. J Foot Ankle Surg. 2007;46:52–54. [PubMed]
3. Biswas S, Murphy M. Subtalar dislocations Internet J Orthoped Surg 2006. 31–5.5Available at http://www.ispub.com/ostia/index.php?xmlFilePath=journals/ijos/vol3n2/subtalar.xml Last accessed July 16, 2008.