Volume 16, Issue 5, September 2015.
Jason D. Heiner, MD
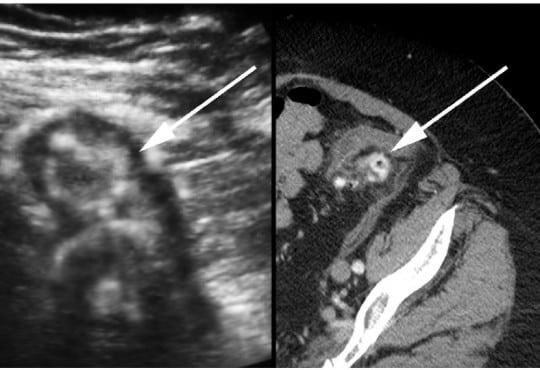
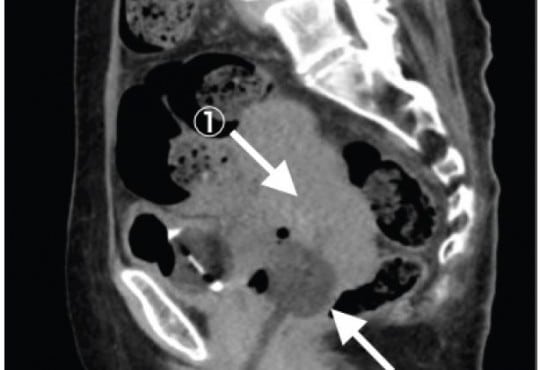
A 72-year-old otherwise healthy female presented to
the emergency department with two weeks of worsening
abdominal pain. She was afebrile with normal vital signs. Her
physical examination was notable for moderate abdominal
tenderness without rebound to the left and suprapubic
regions of the abdomen. Laboratory studies were remarkable
for a white blood cell count of 13,000/mm3
. A focused
bedside ultrasound over the patient’s region of maximal
discomfort revealed a thickened bowel wall and several
small contiguous hypoechoic projections surrounding a
hyperechoic center, suggestive of diverticulitis.
Volume 16, Issue 5, September 2015.
Terri Davis, MSHS, PA-C, et al.
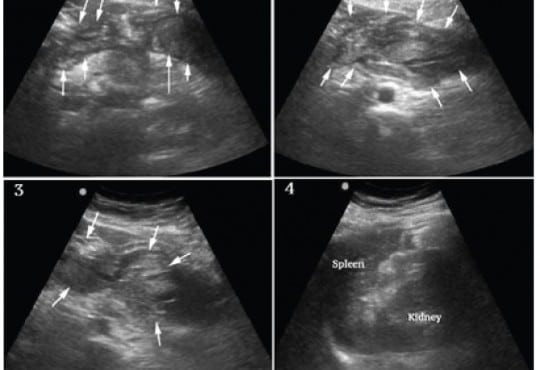
Splenic artery aneurysm rupture is rare and potentially fatal. It has largely been reported in pregnant
patients and typically not diagnosed until laparotomy. This case reports a constellation of clinical and
sonographic findings that may lead clinicians to rapidly diagnose ruptured splenic artery aneurysm
at the bedside. We also propose a rapid, but systematic sonographic approach to patients with
atraumatic hemoperitoneum causing shock. It is yet another demonstration of the utility of bedside
ultrasound in critically ill patients, specifically with undifferentiated shock.
Volume 16, Issue 5, September 2015.
Caroline T. Brandon, MD, et al.
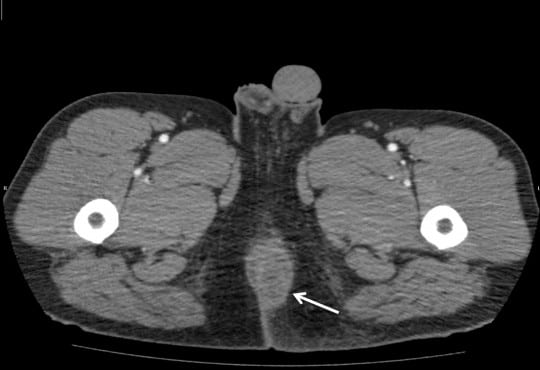
A 34-year-old male with diabetes presented to the
emergency department with four days of progressively
worsening redness, swelling and pain to his left buttock.
The patient denied fevers, chills, rectal pain or purulent
drainage from his rectum. His initial vital signs were heart
rate of 82; blood pressure of 146/92; and temperature of
98.2°F. The left buttock had a poorly circumscribed area of
induration; however, there was no fluctuance or crepitace.
Rectal exam was unremarkable. Because the patient’s
buttock pain was disproportionate to his exam findings,
a point-of-care ultrasound was performed to determine
if a more extensive process was present. The ultrasound
demonstrated cobblestoning, fascial thickening with edema,
and a large 4.5cm fluid collection extending and adjacent
to the rectum.
Volume 16, Issue 5, September 2015.
Mamata V. Kene, MD, MPH, et al.
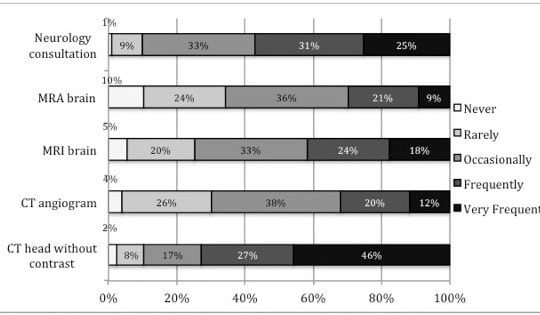
Introduction: We evaluated emergency physicians’ (EP) current perceptions, practice, and attitudes
towards evaluating stroke as a cause of dizziness among emergency department patients.
Methods: We administered a survey to all EPs in a large integrated healthcare delivery system.
The survey included clinical vignettes, perceived utility of historical and exam elements, attitudes
about the value of and requisite post-test probability of a clinical prediction rule for dizziness. We
calculated descriptive statistics and post-test probabilities for such a clinical prediction rule.
Results: The response rate was 68% (366/535). Respondents’ median practice tenure was
eight years (37% female, 92% emergency medicine board certified). Symptom quality and typical
vascular risk factors increased suspicion for stroke as a cause of dizziness. Most respondents
reported obtaining head computed tomography (CT) (74%). Nearly all respondents used and
felt confident using cranial nerve and limb strength testing. A substantial minority of EPs used
the Epley maneuver (49%) and HINTS (head-thrust test, gaze-evoked nystagmus, and skew
deviation) testing (30%); however, few EPs reported confidence in these tests’ bedside application
(35% and 16%, respectively). Respondents favorably viewed applying a properly validated clinical
prediction rule for assessment of immediate and 30-day stroke risk, but indicated it would have to
reduce stroke risk to <0.5% to be clinically useful.
Conclusion: EPs report relying on symptom quality, vascular risk factors, simple physical exam
elements, and head CT to diagnose stroke as the cause of dizziness, but would find a validated
clinical prediction rule for dizziness helpful. A clinical prediction rule would have to achieve a 0.5%
post-test stroke probability for acceptability.
Volume 16, Issue 5, September 2015.
Daniel Miller, MD
Emergency physicians are often required to evaluate and treat undifferentiated patients suffering
acute hemodynamic compromise (AHC). It is helpful to apply a structured approach based on a
differential diagnosis including all causes of AHC that can be identified and treated during a primary
assessment. Tension pneumoperitoneum (TP) is an uncommon condition with the potential to be
rapidly fatal. It is amenable to prompt diagnosis and stabilization in the emergency department. We
present a case of a 16-year-old boy with TP to demonstrate how TP should be incorporated into a
differential diagnosis when evaluating an undifferentiated patient with AHC.
Volume 16, Issue 5, September 2015
Christian Jensen, DO, et al.
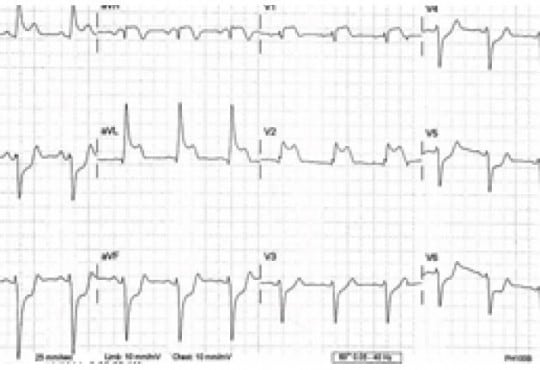
Sumitriptan has been used by millions as a migraine abortant; however, there have been studies
showing angina pectoris, coronary vasospasm, and even myocardial infarction in patients with
predisposing cardiac risk factors. The majority are patients using the injectable form subcutaneously.
We present the case of a patient who presents with ST-elevation myocardial infarction, with no
cardiovascular risk factors, after ingesting oral sumitriptan for her typical migraine.
Volume 16, Issue 5, September 2015
Jill Tirabassi, MD, et al.
A 25-year-old male presented to the ski clinic after
colliding with a tree while snowboarding. He had immediate
sharp pain at his “tailbone,” but denied numbness and
weakness. Past medical history was initially reported as
unremarkable. On exam, he demonstrated midline tenderness
over the sacrum. Pelvic radiography was performed (Figure).
Volume 16, Issue 5, September 2015
Jagdipak Heer, MD, et al.
A 31-year-old gravida 3 Para 3 female with no past
medical history, presented to the emergency department
complaining of a painless “boil” to the right groin, which
had been enlarging for over two months. Although it
was generally painless, she did suffer mild dyspareunia
at times. Antibiotics prescribed by her primary doctor
failed to resolve this mass so she decided to present to the
emergency department.
Volume 16, Issue 5, September 2015.
Stephen L. Thornton, MD, et al.
A previously healthy two-year-old boy presented to the
emergency department with vomiting. He was cyanotic with
mottling of both lower extremities. He was in respiratory
distress with retractions and diminished breath sounds. His
abdomen was distended and rigid. He had a pulse of 170 beats
per minute, blood pressure of 144/69mmHg and respiratory
rate of 42 breaths per minute. He was endotracheally
intubated. Chest and abdominal radiographs demonstrated a
tension pneumoperitoneum.
Volume 16, Issue 5, September 2015.
Richard Slama, MD, et al.
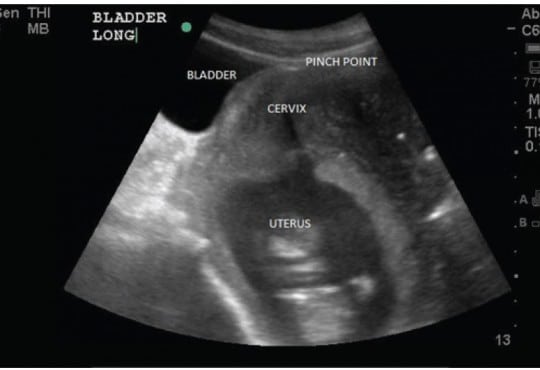
Gravid uterine incarceration (GUI) is a condition that is well discussed in literature; however, there
are few acute diagnoses in the emergency department (ED). We present a case series where
three multiparous females presented to the ED with non-specific urinary symptoms. On bedside
ultrasound, each patient was noted to have a retroverted uterus and inferior bladder entrapment
under the sacral promontory. GUI is a rare condition that can lead to uremia, sepsis, peritonitis, and
ultimately maternal death. Emergency physicians should include GUI in their differential diagnosis in
this patient population and use bedside ultrasound as an adjunct to diagnosis.
Volume 16, Issue 5, September 2015.
Tomohiro Sonoo, MD, et al.
A 67-year-old woman complaining of continuous fresh
vaginal hemorrhage came to our emergency department in a
pre-shock state. Examinations revealed an irregularly shaped
mass in the uterus and active arterial bleeding. Emergent
hysterectomy and interventional radiology were not
immediately available. Foley catheter with 20mL water was
inserted into the uterine cavity, then the balloon was pulled
to obstruct the uterus output (Figure). Her vital signs became
stabilized, and she was transferred to another hospital two
days later.
{kind=link}