
{kind=link}
| Author | Affiliation |
|---|---|
| Conor McKaigney, MD | Queen’s University, Department of Emergency Medicine, Kingston, Ontario, Canada Denver Health Medical Center, Denver, Colorado |
ABSTRACT
Hepatic abscess is an uncommon occurrence in North America, but can be a diagnostic challenge for emergency department physicians. The clinical signs and symptoms may vary, leading to delays in diagnosis and higher morbidity. We present a case of a 35-year old male with a hepatic abscess initially misdiagnosed as pneumonia. On subsequent return to the ED for back pain complaints, a bedside ultrasound led to the appropriate diagnosis. This case report and discussion will attempt to review the literature on the etiology, diagnosis and treatment of hepatic abscess for the emergency physician.
INTRODUCTION
Hepatic abscesses are a relatively uncommon occurrence in North America. They are seen in approximately 2.3 cases per 100,000 with higher rates found among men than women. They do, however, represent a serious risk to patients. Mortality at one time approached 77%, but newer population based studies have estimated rates at closer to 6%.1–3 We present a case of a healthy young patient who presents only with upper back pain, underlining the diagnostic challenge inherent in the disease.
CASE REPORT
A 35-year old male presents to the emergency department (ED) with what he describes as right-sided upper back and flank pain, which he attributes to a “cupping” procedure the day prior. The cupping procedure is an alternative medicine practice that uses local suction to theoretically stimulate blood flow and promote healing. He had no previous issues with the procedure. On further history he reported having had approximately 6 weeks of intermittent fevers, cough, anorexia and general malaise. He had seen multiple naturopathic physicians for these complaints, before an urgent care visit one week earlier. At that time, he had been started on azithromycin and doxycycline for a presumptive diagnosis of pneumonia. In the interim week he reported an improvement in his febrile symptoms and overall well-being. He was an otherwise healthy heterosexual male, without drug use or travel outside the country. He had no known sick contacts.
On physical examination his vital signs included a blood pressure of 116/75 mmHg, a heart rate of 119 beats per minute, and a respiratory rate of 20 breaths per minute. His temperature in the ED was 36.2°C. Oxygen (O2) saturation was 97% on room air. The patient was alert, and appropriate with no signs of respiratory distress. Pertinent physical findings revealed typical, non-tender cupping marks on his back. More concerning was an absence of breath sounds on the right side of the chest on auscultation. His abdomen was soft and non-tender. The remainder of the physical examination was non-contributory.
The initial diagnostic test ordered was a chest radiograph, which showed 80% opacification of the right hemithorax, consistent with pneumonia and associated parapneumonic effusion seen in Figure 1. A bedside ultrasound was subsequently performed in the ED, initially in order to examine the size of the pleural effusion in which a startling discovery was made. The image of the right upper quadrant is shown in Figure 2 and corresponding video clip.
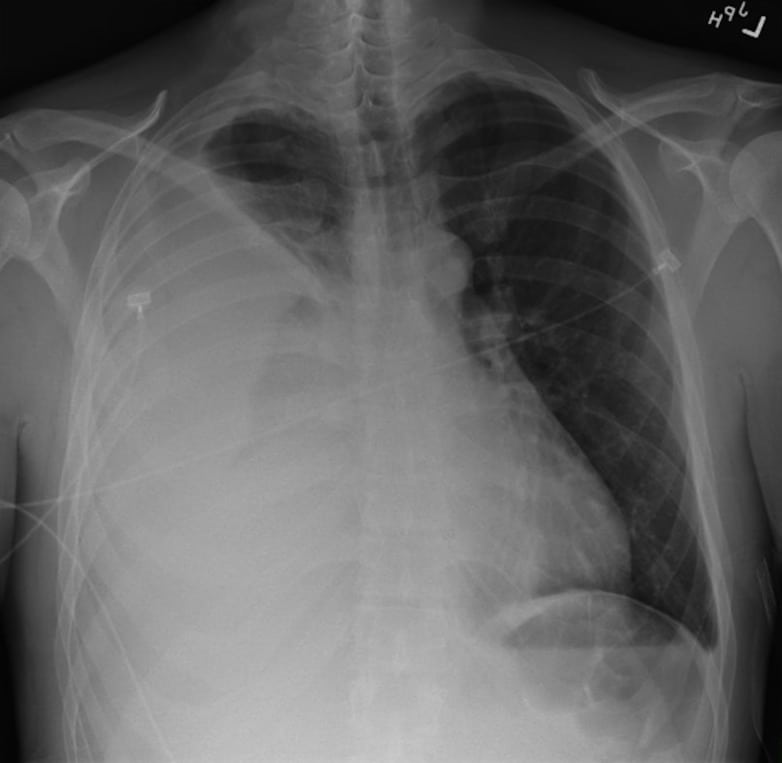
Chest radiograph PA view showing opacification of the right hemithorax.

Bedside ultrasound images showing multiple, hypoechoic, loculated fluid collections within the parenchyma of the liver, consistent with hepatic abscesses. The stars show the boundaries of the cavity. An adjacent hypo-echoic pulmonary effusion can also be seen (circle).
As a result of these abscess findings, the patient underwent a computed tomography (CT) of the chest, abdomen and pelvis to determine the extent of the pulmonary and hepatic disease.
A consultative ultrasound confirms a 10.2 × 8.9 × 12.6 cm abscess in the right lobe of the liver and can be seen in Figure 5. Bloodwork sent after initial examination returned showing a white blood cell count of 25×109/L, creatinine of 92 mmol/L, and lactate of 3.5 mmol/L. Liver transaminases and international normalized ratio were within normal limits. While in the ED his O2 requirements increased to 4L and his blood pressure started to trend down. It dropped to a low of 90/60 with a HR of 108. The patient was treated in the ED with 2 liters of normal saline and started on levofloxacin, vancomycin and piperacillin/tazobactam.
A thoracocentesis was performed showing 33,688 u/L white blood cells with 93% neutrophils although an initial gram stain was negative. Antibiotics were switched to ceftriaxone and metronidazole after infectious disease consultation. The patient was admitted to the surgical intensive care unit where he underwent central line placement and an interventional radiology guided liver abscess drainage with percutaneous drain placement, and tube thoracostomy. He later underwent a video assisted thorascopic surgery (VATS) decortication procedure where a diaphragmatic defect was found, continuous with the hepatic abscess cavity. No microorganisms were found on gram stain, or any subsequent cultures.
Following the VATS procedure the patient made a quick recovery and was discharged from hospital. He continues to recover well. He spent 1 month on intravenous (IV) ceftriaxone and metronidazole administered through a peripherally inserted central catheter line before having the antibiotics discontinued. The etiology of this culture negative abscess has never been identified .
DISCUSSION
The most common cause of hepatic abscess in North America is thought to be from biliary disease.4,5 Abscesses can also develop from hematogenous spread where intestinal disease such as inflammatory bowel disease, diverticulitis, and appendicitis can all seed to the liver via the portal venous system. Even trauma, both blunt and penetrating, has been shown to result in hepatic abscesses in some rare cases. The great majority of abscesses however, develop without a source ever being identified. These are known as cryptogenic abscesses.6
Certain risk factors for abscess development have been described, including recent bowel surgery, diabetes, alcoholism and other immuno-compromised states such as human immunodeficiency virus infections.7
While most hepatic abscesses are monomicrobial, it is not unusual to see polymicrobial infections. In North America, the most common pathogens consistenly identified from abscess cultures areEscherichia coli and Klebsiella sp.8 Interestingly, in a recent Canadian cohort of patients with hepatic abscesses, Strepococcus millieri was the most often cultured organism.1 For patients who have recently visited, or immigrated from developing nations, abscess formation with Entamoeba histolytica can still be seen secondary to fecal-oral contamination.
Generally, patients with hepatic abscess present with fevers and abdominal pain although symptoms can include a broad range of complaints from nausea and vomiting to malaise and weight loss. In some cases, jaundice may be the first and only clinical manifestation of the disease.9 Apart from jaundice, physical examination may show hepatomegaly and right upper quadrant pain although this is seen in only about 50% of cases.6 In some situations hepatic abscess can rupture and spread infection into the thoracic cavity, or even lead to the formation of hepato-bronchial fistulae.10
Bloodwork in patients with hepatic abscesses can also vary, although certain features predominate. The most common laboratory abnormalities are hypoalbuminemia, elevated liver enzyme levels, and leukocytosis.1 Unfortunately no one sign, symptom or laboratory value is specific and the physician must always keep the possibility of hepatic abscess in the differential diagnosis.
The initial radiologic approach to diagnosis often includes a chest radiograph. A chest radiograph may show an elevated hemi-diaphragm, pleural effusion, atelectasis or right lobar consolidation, but is normal in over half of patients.11 The diagnosis of hepatic abscess has been aided greatly by the increase in availability of ultrasonography and CT in the ED. Both are sensitive tests for the detection of hepatic abscess and have contributed to the trend of reduced morbidity.12 Contrast-enhanced CT has slightly increased sensitivity compared with ultrasound and may offer benefit in drainage procedures. Ultrasound is ideal in the initial evaluation of the biliary tree.13 If biliary disease is a suspected source, endoscopic retrograde cholangiopancreatography or magnetic resonance cholangiopancreatography may be indicated. Given these diagnostic options, a multimodal approach is often required for both diagnosis and treatment.
To our knowledge there is only one previous case reporting the use of bedside ultrasound in the diagnosis of a hepatic abscess.13 While use of consultative ultrasound imaging is a standard part of the work up of a suspected hepatic abscess, the test characteristics of bedside ultrasound for hepatic abscess are unknown. Consultative ultrasound has shown a sensitivity range of 86 to 96%.14–16Findings on ultrasound will change depending on the stage of the disease but most commonly include a complex cystic mass with irregular margins and posterior acoustic enhancement. The contents of the structure may take on a more variable echotexture as the untreated abscess progresses where fluid-fluid interfaces and septations become more aparent.14 When gas forming organisms are present, visualization of the abscess itself can be difficult, as air scatters the ultrasound waves giving off a “dirty” appearing shadow that obscures distal structures. These findings should give the bedside ultrasonographer an even higher degree of concern for serious underlying disease.
Treatment of hepatic abscess should include a multi-disciplinary team approach, ideally involving surgery, interventional radiology, and infectious disease specialists. Main treatment goals include drainage of the abscess and antibiotic eradication of the pathogen involved. Initial ED management should follow a goal-directed sepsis protocol, if indicated. Early broad-spectrum antibiotic therapy aimed at the most commonly responsible organisms should be initiated. While obtaining cultures is ideal, they should not delay therapy. There have been multiple antibiotic regimens described but most often should include an extended spectrum B-lactam, or combination of a third generation cephalosporin or fluoroquinolone and metronidazole.6 Of course, local resistance patterns should be considered when initiating antibiotic therapy. Drainage technique may vary depending on surgical expertise and availability of interventional radiology. Some advocate that large abscesses such as those greater than 5cm may benefit from open surgical drainage.17,18 Percutaneous drainage by either ultrasound or CT guided is ideal for most other abscesses.19,20
CONCLUSION
Hepatic abscess is fortunately a relatively uncommon disease in North America as it can be a difficult diagnosis to make. The presenting complaints, physical findings and laboratory markers can be entirely variable as illustrated by our patient. Our case underlines the importance in keeping hepatic abscesses on the differential diagnosis, especially in those patients with the risk factors described. It also serves as a reminder to the ED physician of the ever-expanding utility of bedside ultrasound in the ED.
Footnotes
Supervising Section Editor: Rick A. McPheeters, DO
Submission history: Submitted August 7, 2012; Revision received September 20, 2012; Accepted October 6, 2012
Full text available through open access at http://escholarship.org/uc/uciem_westjem
DOI: 10.5811/westjem.2012.10.13268
Address for Correspondence: Conor McKaigney, MD, PGY-5 Emergency Medicine, Queen’s Univesity, Kingston, Ontario, Canada. Email: 9cjm1@queensu.ca.
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Kaplan GG, Gregson DB, Laupland KB. Population-based study of the epidemiology of and the risk factors for pyogenic liver abscess. Clin Gastroenterol Hepatol. 2004;2:1032. [PubMed]
2. Hansen PS, Schonheyder HC. Pyogenic hepatic abscess: a ten year population-based retrospective study. APMIS. 1998;106:396–402. [PubMed]
3. Ochsner A, DeBakey M, Murray S. Pyogenic abscess of the liver. Am J Surg. 1938;40:292–319.
4. Chen SC, Huang CC, Tsai SJ, et al. Severity of disease as main predictor for mortality in patients with pyogenic liver abscess. Am J Surg. 2009 Aug;198(2):164–172. [PubMed]
5. Huang CJ, Pitt HA, Lipsett PA, et al. Pyogenic hepatic abscess. Changing trends over 42 years. Ann Surg. 1996;223:600–609. [PMC free article] [PubMed]
6. Johannsen EC, Sifri CD, Madoff LC. Pyogenic liver abscesses. Infect Dis Clin North Am.2000;14(3):547Y563. [PubMed]
7. Hernandez JL, Ramos C. Pyogenic hepatic Abscess: clues for diagnosis in the emergency room.Clin Microbiol Infect. 2001;7:567–570. [PubMed]
8. Rahimian J, Wilson T, Oram V, et al. Pyogenic liver abscess: recent trends in etiology and mortality. Clin Infect Dis. 2004;39:1654. [PubMed]
9. Branum GD, Tyson GS, Branum MA, et al. Hepatic Abscess: Changes in Etiology, Diagnosis and Management. Annals of Surgery. 1990;212(6):665–662. [PMC free article] [PubMed]
10. Ala A, Safar-Aly H, Millar A. Metallic cough and pyogenic abscess. Gastroenterology & Hepatology. 2001;13:967, 969. [PubMed]
11. Mohsen AH, Green ST, Read RC, Mckendrick MW. Liver abscess in adults: ten years experience in a UK centre. Q J Med. 2002;95:797–802. [PubMed]
12. Yinnon AM, Hadas-Halpern I, Shapiro M, et al. The changing clinical spectrum of liver abscess: the Jerusalem experience. Postgrad Med J. 1994;70:436–439. [PMC free article] [PubMed]
13. Pearl R, Pancu D, Legome E. Hepatic Abscess. The Journal of Emergency Medicine.2005;28(3):337–339. [PubMed]
14. Benedetti BS, Desser T, Jeffrey RB. Imaging of Hepatic Infections. Ultrasound Quarterly.2008;24:267–278. [PubMed]
15. Malik AA, Bari SU, Rouf KA, et al. Pyogenic liver abscess: changing patterns in approach. World Journal of Gastrointestinal Surgery. 2010;2(12):395–401. [PMC free article] [PubMed]
16. Lin AC, Yeh DY, Hsu YH, et al. Diagnosis of pyogenic liver abscess by abdominal ultrasonography in the emergency department. Emerg Med J. 2009;26:273–275. [PubMed]
17. Tan YM, Chung AY, Chow PK, et al. An appraisal of surgical and percutaneous drainage for pyogenic liver abscesses larger than 5 cm. Ann Surg. 2005;241:485. [PMC free article] [PubMed]
18. Hope WW, Vrochides DW, Newcomb WL, et al. Optimal Treatment of Hepatic Abscess. The American Surgeon. 2008;74(2):178–182. [PubMed]
19. McDonald MI, Corey GR, Gallis HA, et al. Single and multiple pyogenic liver abscesses. Natural history, diagnosis and treatment, with emphasis on percutaneous drainage. Medicine. 1984;63:291.[PubMed]
20. Liu CH, Gervais DA, Hahn PF, et al. Percutaneous hepatic abscess drainage: do multiple abscesses or multiloculated abscesses preclude drainage or affect outcome? J Vasc Interv Radiol.2009;20:1059. [PubMed]