Volume 16, Issue 5, September 2015.
Carlos J. Roldan, MD
Despite the level of skill of the operator and the use of ultrasound guidance, central venous catheter
(CVC) placement can result in CVC malpositioning, an unintended placement of the catheter tip in
an inadequate vessel. CVC malpositioning is not a complication of central line insertion; however,
undiagnosed CVC malpositioning can be associated with significant morbidity and mortality. The
objectives of this review were to describe factors associated with intravascular malpositioning of
CVCs inserted via the neck and chest and to offer ways of preventing, identifying, and correcting
such malpositioning. A literature search of PubMed, Cochrane Library, and MD Consult was
performed in June 2014. By searching for “Central line malposition” and then for “Central venous
catheters intravascular malposition,” we found 178 articles written in English. Of those, we found
that 39 were relevant to our objectives and included them in our review. According to those articles,
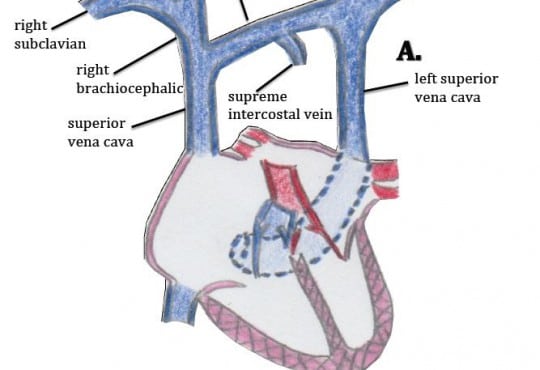
intravascular CVC malpositioning is associated with the presence of congenital and acquired
anatomical variants, catheter insertion in left thoracic venous system, inappropriate bevel orientation
upon needle insertion, and patient’s body habitus variants. Although plain chest radiography is
the standard imaging modality for confirming catheter tip location, signs and symptoms of CVC
malpositioning even in presence of normal or inconclusive conventional radiography findings should
prompt the use of additional diagnostic methods to confirm or rule out CVC malpositioning. With very
few exceptions, the recommendation in cases of intravascular CVC malpositioning is to remove and
relocate the catheter. Knowing the mechanisms of CVC malpositioning and how to prevent, identify,
and correct CVC malpositioning could decrease harm to patients with this condition.
Volume 16, Issue 5, September 2015.
Danielle D. Campagne, MD, et al.
Introduction: The objective is to evaluate the accuracy of medication dosing and the time to
medication administration in the prehospital setting using a novel length-based pediatric emergency
resuscitation tape.
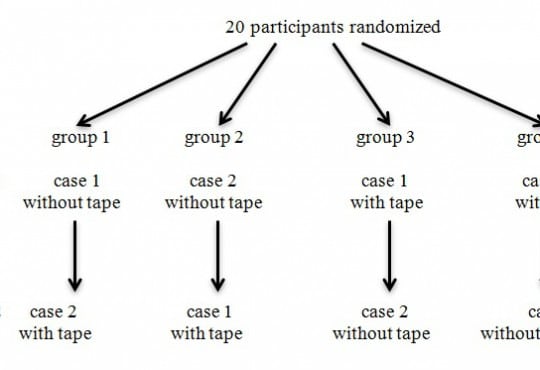
Methods: This study was a two-period, two-treatment crossover trial using simulated pediatric
patients in the prehospital setting. Each participant was presented with two emergent scenarios;
participants were randomized to which case they encountered first, and to which case used the
National Park Service (NPS) emergency medical services (EMS) length-based pediatric emergency
resuscitation tape. In the control (without tape) case, providers used standard methods to determine
medication dosing (e.g. asking parents to estimate the patient’s weight); in the intervention (with
tape) case, they used the NPS EMS length-based pediatric emergency resuscitation tape. Each
scenario required dosing two medications (Case 1 [febrile seizure] required midazolam and
acetaminophen; Case 2 [anaphylactic reaction] required epinephrine and diphenhydramine). Twenty
NPS EMS providers, trained at the Parkmedic/Advanced Emergency Medical Technician level,
served as study participants.
Results: The only medication errors that occurred were in the control (no tape) group (without tape:
5 vs. with tape: 0, p=0.024). Time to determination of medication dose was significantly shorter
in the intervention (with tape) group than the control (without tape) group, for three of the four
medications used. In case 1, time to both midazolam and acetaminophen was significantly faster in
the intervention (with tape) group (midazolam: 8.3 vs. 28.9 seconds, p=0.005; acetaminophen: 28.6
seconds vs. 50.6 seconds, p=0.036). In case 2, time to epinephrine did not differ (23.3 seconds vs.
22.9 seconds, p=0.96), while time to diphenhydramine was significantly shorter in the intervention
(with tape) group (13 seconds vs. 37.5 seconds, p<0.05).
Conclusion: Use of a length-based pediatric emergency resuscitation tape in the prehospital setting
was associated with significantly fewer dosing errors and faster time-to-medication administration in
simulated pediatric emergencies. Further research in a clinical field setting to prospectively confirm
these findings is needed.
Volume 16, Issue 1, January 2015
Katherine Harter, MD et al.
Historically, most patients who required parenteral anticoagulation received heparin, whereas those patients requiring oral anticoagulation received warfarin. Due to the narrow therapeutic index and need for frequent laboratory monitoring associated with warfarin, there has been a desire to develop newer, more effective anticoagulants.
Volume 15, Issue 6, September 2014
Christopher Hahn, MD et al.
Ultrasound-guided nerve blocks are quickly becoming integrated into emergency medicine practice for pain control and as an alternative to procedural sedation. Common, but potentially catastophic errors have not been reported outside of the anesthesiology literature. Evaluation of the brachial plexus with color Doppler should be standard for clinicians performing a supraclavicular brachial plexus block to determine ideal block location and prevention of inadvertant intravascular injection.
Volume 15, Issue 6, September 2014
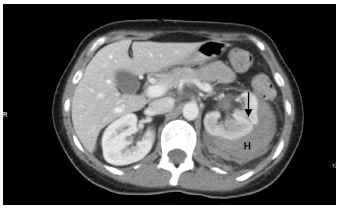
Sam S. Torbati, MD et al.
A 41-year-old woman presented to the emergency department with a chief complaint of hematuria three days status post extracorporeal shockwave lithotripsy. The patient described a three-day history of worsening left-sided abdominal pain immediately following the procedure. She denied any fever, chills, changes in bowel habits, hematochezia, increased urinary frequency, urinary urgency, or dysuria.
Volume 15, Issue 6, September 2014
Rahul Bhat, MD et al.
Emergency physicians frequently perform endotracheal intubation and mechanical ventilation. The impact of instituting early post-intubation interventions on patients boarding in the emergency department (ED) is not well studied. We sought to determine the impact of post-intubation interventions (arterial blood gas sampling, obtaining a chest x-ray (CXR), gastric decompression, early sedation, appropriate initial tidal volume, and quantitative capnography) on outcomes of mortality, ventilator-associated pneumonia (VAP), ventilator days, and intensive care unit (ICU) length-of-stay (LOS).
Volume 15, Issue 4, July 2014
Evelyn Porter, MD et al.
The objective of our study was to estimate the incidence of prescribing medication errors specifically made by a trainee and identify factors associated with these errors during the simulated resuscitation of a critically ill child.
The objective of this study was to evaluate emergency medicine physician and nurse acceptance of nonnurse, nonphysician screening for geriatric syndromes.
{kind=link}