Suicide claimed 47,173 lives in 2017 and is the second leading cause of death for individuals 15–34 years old. In 2017, rates of suicide in the United States (US) were double the rates of homicide. Despite significant research funding toward suicide prevention, rates of suicide have increased 38% from 2009 to 2017. Recent data suggests that emergency medical services (EMS) workers are at a higher risk of suicidal ideation and suicide attempts compared to the general public. The objective of this study was to determine the proportionate mortality ratio (PMR) of suicide among firefighters and emergency medical technicians (EMT) compared to the general US working population.
The COVID-19 pandemic has generated enhanced focus on the safety of healthcare providers and efforts to mitigate the risks of viral transmission.1 Reports of previous viral epidemics have described substantially increased risk to providers performing laryngoscopy and tracheal intubation in patients infected with the virus.
Across the world, efforts are underway to contain the spread and mitigate the impact of COVID-19. These include social distancing efforts such as working from home and meeting via teleconferences.8 The nature of public safety both necessitates that first-responder personnel be present at the station and requires vigilance to keep them healthy to provide essential services to the community. As a result, the fire station represents a front line in the COVID-19 mitigation efforts.
The primary goal of this study was to describe the quantity of and reasons for calls for medical direction. We also sought to determine time diverted from emergency physicians due to OLMD. Finally, we hoped to identify any areas for potential improvement or additional training opportunities for EMS providers.
Most research on drug use occurs in clinics or hospitals; few studies have evaluated the impact of opioid use on emergency medical services (EMS) or the EMS response to opioid use disorder (OUD). This study describes the perceived burden of disease, data collection, and interventions in California local EMS agencies (LEMSA).
We describe our experience treating patients with midazolam for behavioral emergencies in a large urban EMS system. We hypothesized that using midazolam for acute agitation leads to improved clinical conditions without causing significant clinical deterioration.
Timely access to interventional therapy has been linked to improved stroke outcomes. Accurate triage depends upon the use of a validated screening tool in addition to several emergency medical system (EMS)-specific factors. This study examines the integration of a modified Rapid Arterial oCcclusion Evaluation (mRACE) score into an existing stroke treatment protocol.
Our study examines patients who were triaged and admitted to a critical care location, including an intensive care unit (ICU), cardiac catheterization laboratory, or operating room (OR).
Increased out-of-hospital time is associated with worse outcomes in trauma. Sparse literature exists comparing prehospital scene and transport time management intervals between adult and pediatric trauma patients. National Emergency Medical Services guidelines recommend that trauma scene time be less than 10 minutes. The objective of this study was to examine prehospital time intervals in adult and pediatric trauma patients.
We conducted this study to explore the process of violence against EMS providers, using the Strauss/Corbin systematic approach of grounded theory to create a paradigm model. The participants in this research included personnel who had at least two years experience in the EMS systems of the city of Prague and the Central Bohemian Region, and who had been victims of violence.
Under this system, patients reporting a chief complaint of abdominal pain received the closest BLS ambulance dispatched alone emergency if located within three miles of the incident. The objective of this study was to determine the safety of BLS-only dispatch to abdominal pain by determining the frequency of time-sensitive events.
Increasingly, emergency medical services (EMS) systems are deploying prehospital extraglottic airways (EGA) for primary pediatric airway management, yet little is known about their efficacy. We evaluated the impact of a pediatric prehospital airway management protocol change, inclusive of EGAs, on airway management and patient outcomes in children in cardiac arrest or respiratory failure.
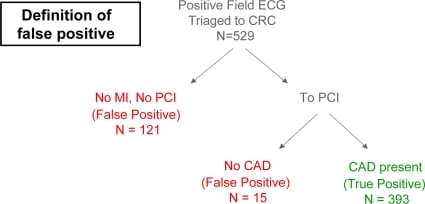
In 2005, Orange County California Emergency Medical Services (EMS) initiated a field 12-lead program to minimize time to emergency percutaneous coronary intervention (PCI) for field-identified acute myocardial infarction (MI). As the program matured, “false-positive” (defined as no PCI or coronary artery occlusion upon PCI) field MI activations have been identified as a problem for the program.
{kind=link}