
{kind=link}
| Author | Affiliations |
| Kenneth A. Scheppke, MD | University of Miami Miller School of Medicine Palm Beach Regional Campus, JFK Medical Center, Department of Emergency Medicine, Atlantis, Florida |
| Joao Braghiroli, MD | University of Miami, Miller School of Medicine, Miami, Florida |
| Mostafa Shalaby, MD | Metrohealth Medical Center Case-Western Reserve University, Department of Hospital Medicine, Cleveland, Ohio |
| Robert Chait, MD | University of Miami Miller School of Medicine Palm Beach Regional Campus, JFK Medical Center, Department of Cardiology, Atlantis, Florida |
Introduction
Methods
Results
Discussion
Limitations
Conclusion
ABSTRACT
Introduction
Violent and agitated patients pose a serious challenge for emergency medical services (EMS) personnel. Rapid control of these patients is paramount to successful prehospital evaluation and also for the safety of both the patient and crew. Sedation is often required for these patients, but the ideal choice of medication is not clear. The objective is to demonstrate that ketamine, given as a single intramuscular injection for violent and agitated patients, including those with suspected excited delirium syndrome (ExDS), is both safe and effective during the prehospital phase of care, and allows for the rapid sedation and control of this difficult patient population.
Methods
We reviewed paramedic run sheets from five different catchment areas in suburban Florida communities. We identified 52 patients as having been given intramuscular ketamine 4mg/kg IM, following a specific protocol devised by the EMS medical director of these jurisdictions, to treat agitated and violent patients, including a subset of which would be expected to suffer from ExDS.
Twenty-six of 52 patients were also given parenteral midazolam after medical control was obtained to prevent emergence reactions associated with ketamine.
Results
Review of records demonstrated that almost all patients (50/52) were rapidly sedated and in all but three patients no negative side effects were noted during the prehospital care. All patients were subsequently transported to the hospital before ketamine effects wore off.
Conclusion
Ketamine may be safely and effectively used by trained paramedics following a specific protocol. The drug provides excellent efficacy and few clinically significant side effects in the prehospital phase of care, making it an attractive choice in those situations requiring rapid and safe sedation especially without intravenous access. [West J Emerg Med. 2014;15(7):736-741.]
INTRODUCTION
It is not uncommon for paramedics and emergency medical technicians (EMTs) to be confronted with combative, violent and uncooperative patients. A subset of these patients will exhibit aggressive behavior, altered sensorium, and may demonstrate hyperthermia, “super human” strength, diaphoresis and a lack of willingness to yield to overwhelming force. Moreover, a certain percentage of these individuals will go on to expire from sudden cardiac arrest. Originally classified as “agitated delirium” or “excited delirium” by the forensic community, the term has now been adopted by the emergency medicine, psychiatric, law enforcement and prehospital literature. Recently, a task force convened by the American College of Emergency Physicians has coined the phrase excited delirium syndrome (ExDS) to cover those patients with altered mental status who demonstrate severe agitation and combative or assaultive behavior.1
The management of ExDS is also difficult and the associated mortality warrants further study. The ability to gain “medical” control of these patients and allow resuscitative therapy to be administered is of the utmost importance. Many different medications can be given to effect sedation in the pre-hospital field including benzodiazepines, haloperidol and others. Many of the medications commonly used are far from ideal in that their onset of action is not immediate, the intravenous (IV) route is often preferred and, when given in the higher dosages required to adequately sedate violent patients, negative hemodynamic and respiratory side effects can make their use potentially harmful for the patient. Previous feedback obtained from local paramedic experience revealed a perceived lack of timely efficacy with haloperidol and benzodiazepine use in the field. The ideal medication, if one exists, would be given intramuscularly, have a near-immediate onset of action, a high efficacy rate even with the most violent and agitated patients, and have zero negative hemodynamic and respiratory side effects. With this as a background and due to the scant literature available, the medical director of five different municipal Fire/Rescue agencies (K.S.) developed a protocol for paramedics to administer intramuscular ketamine (Figure). Furthermore, it is well known that ketamine can cause an emergence reaction; therefore, midazolam was also to be administered to help avoid this potential reaction, but not for its sedative effects.
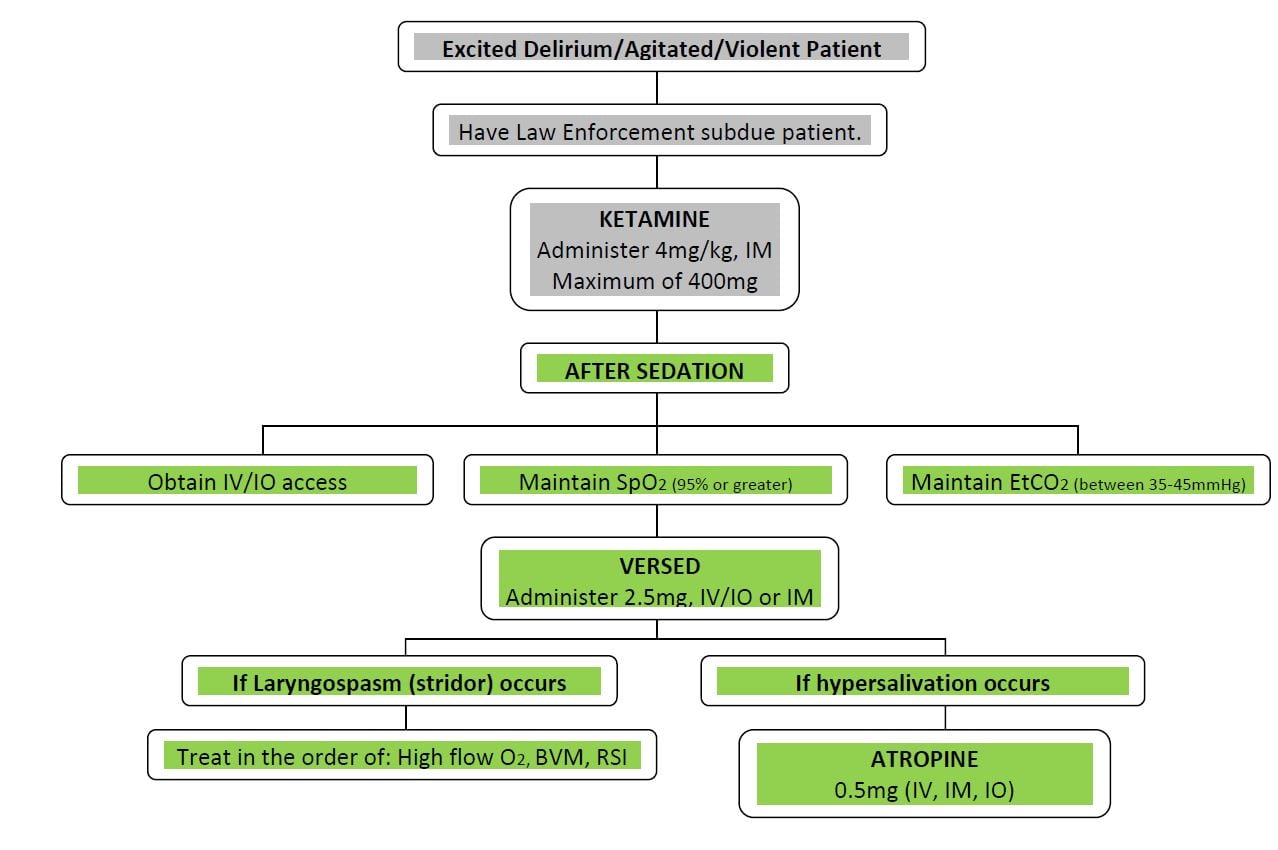
Figure. Prehospital ketamine protocol flowchart.
IM, intramuscular; IV, intravenous; IO, intraosseous infusion; EtCO2, end tidal CO2; BVM, bag-valve-mask; RSI, rapid sequence intubation
METHODS
We retrospectively screened paramedic run sheets from January 1, 2011 through May 1, 2014 for cases where the ketamine protocol was used for complaints of violent, aggressive behavior secondary to a psychiatric or substance-abuse issue. Reviewing the run sheets generated from these encounters we (R.C.) investigated the apparent benefits and risks of intramuscular ketamine given to sedate violent and agitated patients in the field. Approval from the university Institutional Research Board was obtained to review those records.
The medical director of several municipal fire/rescue agencies in Palm Beach County Florida (Boynton Beach Fire Rescue, Palm Beach Gardens Fire Rescue, Greenacres Fire Rescue, Town of Palm Beach Fire Rescue, and West Palm Beach Fire Rescue) has the authority and responsibility to develop medically correct standing orders for paramedics to use while treating patients in the prehospital setting.2
Under this authority, and in response to continuous feedback from paramedic crews about the difficulty and lack of success in dealing with and subsequently treating patients with violent or agitated behavior, a protocol was developed to allow rapid chemical restraint of these patients (including suspected ExDS) through the use of ketamine given as a single intramuscular injection at a dose of 4mg/kg of estimated body weight (Figure).
After initial sedation and control of the patient with ketamine, and per protocol, if possible, an intravenous line was established and a recommended dose of 2.0-2.5mgs of midazolam was given to prevent the well known but infrequent occurrence of a ketamine-induced emergence reaction.3 Following appropriate chemical restraint, treatment of the underlying medical problem was to be initiated in the standard manner and the patient was transported to the closest appropriate hospital per protocol. We obtained cases where use of the ketamine sedation protocol occured from the above noted fire/rescue agencies from January 1, 2011 through May 1, 2014 and reviewed these reports. As a matter of routine paramedic practice, several sets of vital signs were obtained during transport, and any adverse hemodynamic or respiratory effect of the ketamine was noted on the paramedic run sheet.
The primary endpoint was to determine if ketamine provided adequate sedation of sufficient duration to effectively treat and transport these patients to a receiving hospital. Two additional endpoints were the amount of time it took to obtain “medical control” of these patients and whether there were any untoward hemodynamic or respiratory side effects noted from the use of the drug. We defined “medical control” as an adequate level of sedation to allow standard transport and treatment without further violence or agitation. Untoward hemodynamic effects was defined as any resuscitation needed for systolic blood pressure below 90. We defined untoward respiratory effects as any intervention requiring positive pressure ventilation.
RESULTS
A total of 52 patients with violent or agitated behavior were treated from the five service areas during the specified time period. The most common causes of the agitated and aggressive behavior (as noted by the paramedics) was either documented or suspected substance abuse and psychiatric emergencies (Table).
Table. Characteristics and demographics of patients with violent or agitated behavior treated with ketamine by paramedics.
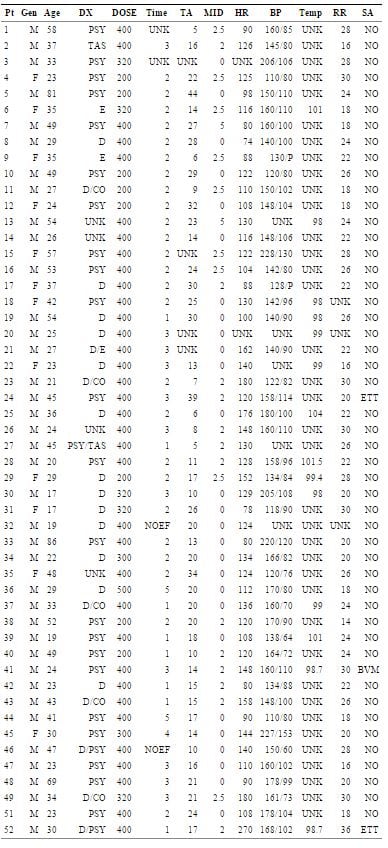
DX, diagnosis by paramedics; DOSE, ketamine dose in mg; Time, time to sedation; TA, time to arrival at hospital; MID, midazolam dose in mg; HR, heart rate; BP, blood pressure initially; T, temperature; RR, respiratory rate; SA, side effects from ketamine noted; TAS, Taser; D, Drug reaction; E, ETOH; Psy, psychiatric problem; CO, cocaine; UNK, no documentation; NOEF, no effect; BVM, bag valve mask required; ETT, required intubation.
The average dose of ketamine used was 4 mg/kg and suitable sedation was obtained in every case but two (96%). Excluding the two ineffective uses, time to achieve effective sedation and medical control averaged just over two minutes. There were three cases (6%) of significant respiratory depression. One case required brief use of a bag valve mask, and two cases endotracheal tube intubation. Of note, in all three cases where respiratory depression was noted, the patients had also received midazolam. The average time to arrival to the emergency department from the time of injection was just under 19 minutes and, aside from the two ineffective uses, sedation was still present in every case. Nearly half of the patients did receive midazolam at a dose between 2-2.5mg either IV or intramuscular (IM) following or concurrently with the administration of the ketamine IM.
DISCUSSION
Psychomotor agitation occurs via several mechanisms. Cocaine causes an increase in the central nervous system excitatory amino acids glutamate and aspartate, and release of the excitatory neurotransmitters norepinephrine, serotonin, and dopamine. The hyperthermia seen in cocaine-intoxicated patients is directly related to the extent of their psychomotor agitation and the ambient temperature.4
Cocaine-associated agitated delirium is a syndrome of hyperthermia with delirium and severe agitation that can progress to respiratory arrest and death. Restrained patients appear to be at particularly high risk with this syndrome.5-10 The pathophysiology of cocaine-associated agitated delirium is a complex process involving down-regulation of dopamine receptors with subsequent dopamine excess during times of cocaine binges.9,11-13 When patients with cocaine or other stimulant- associated agitated delirium are restrained, especially in the prone position, interference with normal respiratory mechanics increases the likelihood of hypoventilation, hypercarbia, acidemia and hypoxemia, ultimately leading to asphyxia and death. It has also been suggested that excessive muscle activity producing lactic acidosis is an additional exacerbating factor. Additionally, stress caused by the restraining process may increase the risk of fatal cardiac arrhythmias due to catecholamine surge in an already cocaine-sensitized myocardium.9-11
Ketamine is a phencyclidine derivative that causes dissociation between the cortical and limbic systems, which prevents the higher centers from perceiving visual, auditory or painful stimuli. It has a rapid onset and a short duration of action and produces significant sedation and analgesia.
There is no consensus about which of many available medications is the best to manage the prehospital agitated or violent patient. Route of administration along with potential for untoward side effects must be weighed when choosing which agent to use. Intramuscular agents are attractive due to their relative ease of administration in a violent patient; however rapidity of onset of sedation is equally important.
Prehospital determination of which patients require sedation also has a range of criteria. A study by the Israel Defense Force uses the inability to place a pulse oximeter on the patient to rule out hypoxemia as an indication for sedation.14 In that study of 18 patients, several patients received ketamine intravenously. In our study only intramuscular ketamine was given, and suitable sedation was achieved in every case but two. There were no reported signs of emergence reaction noted during the prehospital portion of care; however, this case series was not designed to determine if any developed later in the course of hospital treatment.
Ketamine is a potentially ideal drug for prehospital sedation as it has an excellent safety profile, potent anesthetic effects and rapid onset of action with an absence of respiratory depression and a short duration of action. In all but three cases it was felt that the drug was effective in three minutes or less, in two cases the time to effective sedation could not be extrapolated from the run report and in two cases it failed to achieve adequate sedation. There have been previous reports on the use of ketamine in the prehospital setting.15 The drug provides effective analgesia and amnesia to pain and events. There are minimal cardiovascular effects. A previous study by Porter demonstrated the drug may be safely used by non-physician personnel.16 Ketamine also has dissociative properties that can be induced with 1-2mg/kg intravenously (IV) or 4-5mg/kg intramuscularly. Duration of action is typically 10-15 minutes when administered IV and 20-30 minutes when given IM. The dissociative state has no progressive depth nor level and is either present or not, and additional doses do not enhance or deepen the sedation. Thus, adequate sedation can be reliably and safely achieved with one dose even without IV access. Ketamine has been used in burn patients, long bone fractures, other traumatic problems and multiple medical problems, as well as pre-procedural sedation, all of which suggests a wide range of potential beneficial uses for this agent.17
Our study demonstrated the use of ketamine by paramedics to be safe. This is consistent with ketamine’s track record of safety, including reports where inadvertent overdoses of 5 to 100 times the intended dose demonstrated no adverse outcomes.18 In the three cases where respiratory sedation required paramedic intervention, it was co-administered with midazolam, suggesting that extra caution with regard to airway management must be given when using both medications simultaneously.
While we find that ketamine worked well in our study, our evaluation also revealed some sedation protocol violations. Several patients, while noted to be very agitated, did not have their temperatures taken. It is recognized that in these violent patients, obtaining full vital signs is not always readily achievable. However, this also represents an educational opportunity for the paramedics regarding the ExDS and the importance of ruling out hyperthermia and its consequences after chemical restraint allows a more complete evaluation. In addition, approximately half of the patients did not receive a post-ketamine dose of midazolam to help prevent potential emergence reactions, yet they were adequately sedated for the entire transport. Paramedics interviewed by one of the authors (K.S.) regarding this apparent repeated protocol violation, revealed that midazolam was frequently omitted by some paramedics due to the excellent sedation routinely achieved by ketamine alone and therefore the feeling that further sedation with midazolam was unnecessary, while others adminstered it routinely despite excellent sedation because it was in the protocol. Given the three cases of respiratory depression that occurred with the co-administration of midazolam, the excellent sedation with ketamine alone, and the sole use of midazolam in the protocol as prophylaxis for possible emergence reactions, this suggests that further sedation with a benzodiazepine could potentially be delayed until hospital arrival.
LIMITATIONS
This was an uncontrolled observational study with a limited number of subjects. As such, care needs to be taken in generalizing from this study. While the literature is limited, there is evidence that the use of ketamine in the prehospital setting is an effective and safe practice with multiple benefits. We have shown that paramedics, given appropriate training and following a protocol, can administer the drug to violent and agitated patients with great success and minimal risk. An additional limitation of the study is in the selection process for patients to review. While the authors believe the vast majority of ketamine uses have been entered into the data set, it is possible some cases were not discovered owing to the retrospective nature of the chart review. Another potential limitation of the study is reliance on documentation of side effects by paramedics. While it is recognized that the management of these patients is very difficult, it is interesting to note that there was a significant amount of missing data on the run sheets, which may have also played a role in our analysis. However, while the lack of some documentation by paramedics may be an issue, it probably does not alter the important aspects of this study, as any severe side effect would require an intervention such as intubation that would otherwise mandate documentation.
CONCLUSION
This study demonstrates that IM ketamine in the prehospital setting is a good choice to gain rapid medical control of patients with potential ExDs and those exhibiting violent and agitated behavior. A prospective head-to-head trial of ketamine versus other drugs should be carried out with clearly defined endpoints to fully delineate which therapeutic regimen is best for the rapid sedation and control of this difficult-to-manage patient population.
ACKNOWLEDGEMENTS
The authors would like to thank the firefighter/paramedics and chiefs of the following departments, without whose help this article would not be possible: Boynton Beach Fire Rescue, Palm Beach Gardens Fire Rescue, West Palm Beach Fire Rescue, Greenacres Fire Rescue, Town of Palm Beach Fire Rescue.
Footnotes
Supervising Section Editor: Jeffrey Suchard, MD
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Kenneth A. Scheppke, MD, 5301 South Congress Avenue, Atlantis, Fl 33462. Email: kenneth.scheppke@shcr.com.
Submission history: Submitted July 17, 2014; Accepted September 4, 2014
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
- Vilke GM, DeBard ML, Chan TC, et al. Excited delirium syndrome (ExDS): defining based on a review of the literature. J Emerg Med. 2012;43(5):897-905.
- Florida Satutes Chapter 401 and Rule 64-J Florida Administrative Code.
- Patel Piyush, Patel Hemal, Roth David. General Anesthetics and Therapeutic Gases In: Laurence Brunto, Bruce Chabner, Bjorn Knollman eds. Goodman and Gilman The Pharmacologic Basis of Therapeutics. New York NY McGraw Hill Companies.
- Marzuk PM, Tardiff K, Leon AC, et al. Ambient temperature and mortality from unintentional cocaine overdose. JAMA. 1998;27(22):1795.
- Lavoie FW. Consent, involuntary treatment and the use of force in an urban emergency department. Ann Emerg Med. 1992;21:25.
- Stratton SJ, Rogers C, Green K. Sudden death in individuals in hobble restraints during paramedic transport. Ann Emerg Med. 1995;259:710-12.
- Glatter K, Karch SB. Positional asphyxia: inadequate oxygen or inadequate theory? Forensic Sci Int. 2004;141:201-2.
- Pollanen MS, Chiasson DA, Cairns JT. Unexpected death related to restraint for excited delirium: a retrospective study of deaths in police custody and the community. CMAJ. 1998;12:1603.
- Wetli CV, Fishbain DA. Cocaine-induced psychosis and sudden death in recreational cocaine users. J Forensic Sci. 1985;30:873.
- Alshayd H, Showkat A, Wall BM. Lactic acidosis in restrained cocaine intoxicated patient. Tenn Med. 2010;103:37-9.
- Ho J, Dawes DM, Moore JC, et al. Effect of position and weight force on inferior vena cava diameter-implications for arrest-related death. Forensic Sci Int. 2011;22:256-9.
- Hick JL, Smith SW, Lynch MT. Metabolic acidosis in restraint-associated cardiac arrest: a case series. Acad Emerg Med. 1999;6:239.
- Staley J, Basile M, Wetli C et al. Differential regulation of the dopamine transporter in cocaine overdose deaths. NIDA Res Monogr. 1994;141:32.
- Staley JK, Hearn WL, Ruttenber AJ, et al. High affinity cocaine recognition sites on the dopamine transporter are elevated in fatal overdose victims. J Pharm Exp Ther. 1994;271:1678.
- Melamed E, Oron Y, Ben-Avraham R, et al. The combative multi-trauma patient: a protocol for pre-hospital management. Eur J Emer Med. 2007;14:265-68.
- Svenson JE, Abernathy MK. Ketamine for pre-hospital use: new look at an old drug. Am J Emer Med. 2007;25:977-80.
- Green SM, Roback MG, Kennedy RM, et al. Clinical practice guideline for emergency department ketamine dissociative sedation: 2011 update. Ann Emerg Med. 2011;57:449-61.
- Porter K. Ketamine in pre-hospital care. Emerg Med J. 2004;21:351-4.