
{kind=link}
| Author | Affiliation |
|---|---|
| Rob Stephenson, PhD | Emory University, Rollins School of Public Health, Hubert Department of Global Health, Atlanta, GA |
| Christopher Rentsch | Emory University, Rollins School of Public Health, Department of Epidemiology, Atlanta, GA |
| Laura F Salazar, PhD | Emory University, Rollins School of Public Health, Department of Behavioral Science and Health Education, Atlanta, GA |
| Patrick S Sullivan, DVM, PhD | Emory University, Rollins School of Public Health, Department of Epidemiology, Atlanta, GA |
ABSTRACT
Introduction:
Although the research community has begun to recognize intimate partner violence (IPV) as an important issue in same-sex relationships, there has been a lack of attention to characteristics of these relationships that may be associated with IPV. In particular, there has been a lack of attention paid to the associations between dyadic characteristics and IPV in same-sex relationships. This paper examined associations between dyadic characteristics, including relationship satisfaction, communal coping and efficacy, and perpetrating and experiencing IPV among a sample of United States men who have sex with men (MSM).
Methods:
We collected data via an online survey with 528 MSM, who were greater than 18 years of age and reported at least one male sex partner in the last 12 months. The analysis examined dyadic factors associated with reporting of experiencing and perpetrating emotional violence, physical violence, and sexual violence.
Results:
The prevalence of violence in the sample ranged from nine percent reporting perpetrating sexual violence to 33% of men reporting experiencing emotional violence. MSM who reported greater satisfaction with their relationship or who reported a higher degree of concordance with their partner on lifestyle choices were less likely to report experiencing or perpetrating emotional violence. MSM who perceived a stigma to being in a male same-sex couple were less likely to report experiencing or perpetrating sexual violence.
Conclusion:
The results presented here demonstrate high levels of IPV among MSM and that dyadic characteristics are associated with the occurrence of IPV. Understanding relationship characteristics associated with increased IPV among same-sex male couples can contribute to the development of more accurate IPV screening tools, and more sensitively and appropriately designed intervention messages.
INTRODUCTION
In the scientific literature, the most common depiction of intimate partner violence (IPV) involves a male batterer and a female victim. However, IPV is not a problem exclusive to heterosexual relationships. A growing body of literature suggests that IPV occurs within same-sex relationships and that the members of lesbian, gay, bisexual and transgender (LGBT) communities face a number of unique challenges in accessing IPV-related services.1,2 Based on Unites States (U.S.) census data, approximately 700,000 same-sex couples cohabit in the U.S. as of 2004.3 Same-sex intimate partners may be defined as two persons of gay, lesbian or bisexual sexual orientation who currently share an important affective interpersonal relationship, typically characterized by romantic, emotional or sexual connections.4 In many states, same-sex partnerships are not recognized legally, and thus couples may have limited or no access to traditional IPV safeguards (e.g. civil protective orders).5,6 Additionally, a number of methodological issues have hampered research into IPV among LGBT individuals.7 These include a tendency to focus on lesbians, often to the exclusion of gay and bisexual men, a focus on child abuse and hate crimes to the exclusion of IPV and a failure to use representative samples. The latter is due to the problems researchers have faced in recruiting representative samples, and many researchers have thus relied upon convenience samples recruited through LGBT publications, events and organizations.8,9 Moreover, statistics regarding same-sex IPV from service providers may not be comprehensive. Victims of same-sex IPV may be hesitant to seek help, due to internalized or institutionalized homophobia, the nature of the abuse itself, or a perceived lack of useful resources resulting in underreporting of abuse.10–13 The current research examines the prevalence of IPV among an internet-based sample of men who have sex with men (MSM) in the U.S. and explores the associations between dyadic factors and the reporting of sexual, physical and emotional violence. An understanding of how dyadic characteristics shape the reporting of violence not only adds significantly to the small body of literature on same-sex IPV, but also provides valuable information to inform the development of more accurate and perhaps culturally sensitive screening tools and prevention messages for IPV in same-sex couples.
The existing evidence suggests that IPV affects approximately one-quarter to one-half of all same-sex relationships.2,9,10,14 These rates are similar to estimates of abuse in heterosexual relationships.10 The National Coalition of Anti-Violence Programs, reported 6,523 cases of IPV in LGBT relationships in 2003, with most cases (83%) occurring in gay and lesbian relationships. 15Physical abuse seems to occur in a significant portion of abusive same-sex relationships. Elliot16 and De Vidas17 suggest that between 22–46% of lesbians have been in relationships in which physical violence has occurred. McClennen et al.,1 using a sample of 63 gay men, found that participants were often physically struck by their partners and coerced into substance abuse. Greenwood et al.,18reported that 22% of a sample of men who had sex with men had been subjected to physical abuse from an intimate partner. Research also indicates that sexual abuse is common in IPV-afflicted same-sex relationships. Walder-Haugrud and Gratch19 reported that 52% of their sample of gay men experienced one or more incidents of sexual abuse. Similarly, Toro-Alfonso and Rodriques-Madera20 found that approximately 25% of a sample of Puerto Rican gay males had experienced sexual coercion. Clearly, a large number of same-sex relationships experience IPV, and the levels experienced appear to be similar, if not higher, than those seen in heterosexual couples.16
IPV in same-sex couples shares much in common with IPV in heterosexual couples.21,22 For example, both may involve similar reasons for the victim remaining in an abusive relationship (e.g. fear of further abuse, financial dependency), and the use of alcohol as a precipitant to aggressive acts.23 Blosnich24 reports that gay men report experiencing more sexual and verbal violence than heterosexual men, and gay men also tend to report more victimization in casual relationships than is experienced by heterosexual men. However, researchers have yet to establish the extent to which the dynamics of violent same-sex relationships are similar to those found in violent heterosexual relationships.25
Bartholomew and Cobb26 developed a dyadic model of partner violence, which describes how individual and dyadic factors, both individually and jointly, shape the risk of violence in heterosexual couples. The model has four sets of factors: background/depositions (family background, personality and psychopathology), relationship context (power imbalance, relationship discord), situational context (dyadic interaction, inhibition of aggression) and pattern of partner violence (severity, mutuality). The model argues that regardless of individual dispositions towards violence, partners in mutually satisfying relationships, characterized by trust and constructive communication, would not be at risk for IPV. However, although it seems plausible to suggest that the same may hold true for same-sex relationships, studies to date have not examined how dyadic characteristics are associated with the reporting of IPV in same-sex couples.
Using data from an internet-recruited sample of MSM in the U.S., this paper examined the dyadic characteristics associated with experiencing and perpetrating emotional, physical and sexual IPV among male same-sex couples. The analysis focused on the associations between relationship satisfaction, perceived couple-level efficacy, communal coping to prevent Human Immunodeficiency Virus (HIV), and perceived relationship support and experiencing or perpetrating IPV. Understanding the dyadic characteristics associated with experiencing or perpetrating IPV has the potential to significantly inform the design and development of interventions and messages aimed at reducing IPV in the LGBT population.
METHODS
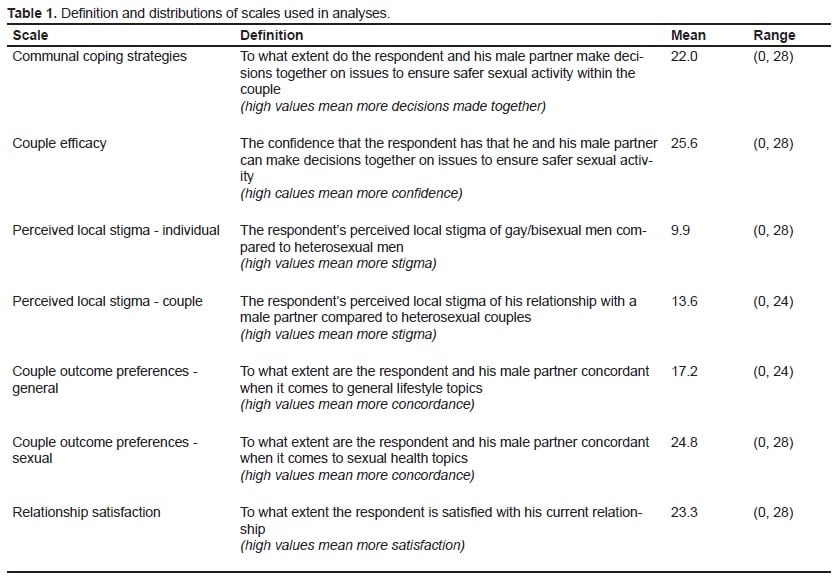
We collected data from internet-using MSM through selective placement of banner advertisements on Facebook.com in May and July, 2010. Advertisements were displayed to Facebook members based on self-reported demographic profile information (male sex and reported interest in men). Exposures were made to the profiles of men greater than or equal to18 years of age logging into Facebook, whose profiles indicated residence in the U.S., reported being in a relationship and having an interest in men. Participants who clicked through the banner advertisements were taken to an internet-based survey where they were first screened for eligibility. Participants were eligible to complete the survey if they were male, greater than18 years of age, reported at least one male sex partner in the last 12 months, and currently had a main male sex partner. Eligible participants were provided informed consent documents and consenting participants were given access to the online survey. In the survey, participants were asked about demographic information (age, education, occupation, race and ethnicity) and recent sexual behaviors (including number and gender of partners and condom use). We included several dyadic constructs derived from both interdependence theory and communal coping perspectives: frequency of using communal coping strategies, couple efficacy, perceived stigma around their relationship, and current relationship satisfaction. 27 We created seven scales to measure these dyadic characteristics (Table 1). Scale items were informed by qualitative data collected with gay men in Atlanta, Chicago and Pittsburgh. We conducted six focus group discussions where men were asked about their current relationships, how they determined relationship satisfaction, their perceived support for their relationships within their community, the methods used by men in same-sex relationships to cope with health or financial threats, their decision-making process with their partner, and their degree of confidence that they could work with their partner towards a shared goal.
We used the Conflict Tactics Scale Revised to assess both perpetration and experience of IPV.28Experiencing emotional IPV was assessed with four of the Psychological Abuse subscale items: he “called me fat or ugly;” “destroyed something belonging to me;” “accused me of being a lousy lover;” or “threatened to hit or throw something at me.” Experiencing physical IPV was assessed with six items: he “threw something at me that could hurt;” “pushed or shoved me;” “punched or hit me with something that could hurt;” “slammed me against a wall;” “beat me up;” or “kicked me.” Experiencing sexual IPV was assessed with three items: he “made me have sex without a condom;” “used force (like hitting, holding down, or using a weapon) to make me have oral or anal sex;” or “used threats to make me have oral or anal sex.” Men were also asked if they had perpetrated any of these forms of IPV against their current male partner, using the same definitions. We create six binary variables to capture prevalence of experiencing and perpetrating each form of IPV (emotional, physical and sexual).
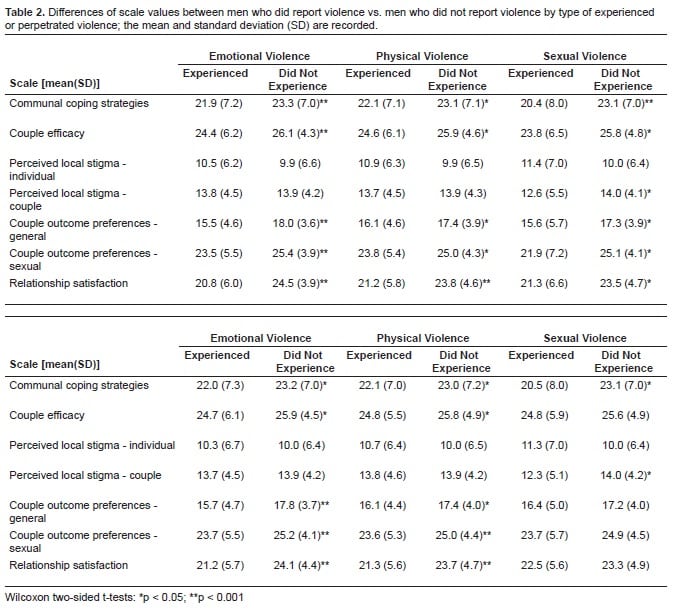
Of the 2,570 men who responded to the advertisements, 1,927 completed screening. Of those, 1,387 were eligible, 1,376 (99%) consented to participate. As is typical of lengthy online surveys, only about half (664) of those who consented completed the survey; of those, 656 (99%) answered the questions on IPV and 528 (80%) completed questions for all covariates of interest; thus, our final sample size used for analyses was 528. We performed two-sided Wilcoxon rank-sum tests and chi-square (χ2) tests to examine differences in dyadic characteristics between those who reported IPV and those who did not report IPV (Table 2).
Separate logistic models were fitted for each of the binary IPV variables. The six outcomes were experiencing or perpetrating emotional violence (EEV or PEV), experiencing or perpetrating physical violence (EPV or PPV) and experiencing or perpetrating sexual violence (ESV or PSV). The key covariates of interest in each of the models were the seven scales measuring the dyadic characteristics: regression models also controlled for demographic variables, such as age, partner’s age, race, education level and HIV status. We conducted co-linearity assessments to verify the stability of the regression models. The research was approved by Emory University’s institutional review board. We conducted analyses with SAS 9.2, Cary, NC.
RESULTS
Respondents were mostly white (84%), HIV-negative (90%) and had at least some college education (82%). Reported ages ranged from 18 to 71-years-old, with a median age of 27. Most men (64%) reported that their male partner’s age was within five years of their own. Figure 1 shows the prevalence of the six types of IPV within the sample: 33% of men reported experiencing emotional violence from a male partner, 23% reported experiencing physical violence, and 10% reported experiencing sexual violence. The prevalence of reported perpetration of violence was lower than the reported experience of violence, with 30% reported perpetrating emotional violence towards a male partner, 20% reported perpetrating physical violence, and nine percent reporting perpetrating sexual violence.
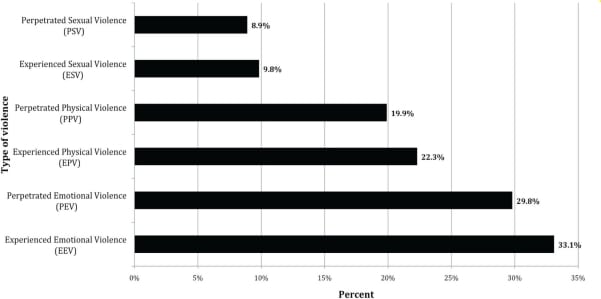
Table 2 shows the differences in dyadic characteristic between men who did and did not report IPV. With the exception of perceived local stigma – individual, all scale values were lower among men who reported IPV. Men who reported experiencing emotional, physical or sexual violence had significantly lower levels of reporting of communal coping strategies, couple efficacy, couple outcome preferences and relationship satisfaction than men who did not experience violence. Men who reported experiencing sexual violence also had significantly higher values on the scale measuring perceived local stigma around their relationship. Men who reported perpetrating emotional or physical violence had lower reported levels of communal coping, couple efficacy, couple outcome preferences and relationship satisfaction than men who did not perpetrate these types of violence. In addition, men who reported perpetrating sexual violence had lower communal coping scores and higher perceived local stigma around their relationship than men who did not report perpetrating sexual violence.
Table 3 shows the results of the modeling of the IPV outcomes. There were no significant associations between age or partner age difference and any of the six IPV outcomes. Men who reported they were HIV-positive were significantly more likely to report perpetrating physical IPV (OR 2.25 95%CI 1.13, 4.48) and to report experiencing sexual violence (OR 2.44, 95%CI 1.05, 5.69). Men with college education were less likely than men with only high school education to report experiencing emotional violence (OR 0.46, 95%CI 0.24, 0.86), perpetrating emotional violence (OR 0.33, 95%CI 0.17, 061), experience sexual violence (OR0.34, 95%CI 0.13, 0.85) and to report perpetrating sexual violence (OR0.30, 95%CI0.12, 0.73). Respondents reporting a racial identity other than white were more likely (OR2.01, 95%CI1.11, 3.67) to report experiencing physical violence than white respondents.

Respondents who reported higher levels of relationship satisfaction were less likely to report experiencing emotional violence (OR 0.90, 95%CI 0.85, 0.95), perpetrating emotional violence (OR 0.92, 95%CI 0.88, 0.97), and to report experiencing physical violence (OR0.93, 95%CI 0.88, 0.98). Respondents who scored high on the couple outcome preferences-general scale, and thus felt they had a high degree of concordance with their partner on lifestyle topics, were less likely to report experiencing emotional violence (OR 0.94, 95%CI 0.88, 1.00) and to report perpetrating emotional violence (OR 0.92, 95%CI 0.87, 0.98). Men who scored high on the perceived local stigma-couple score, and thus reported a perception of more stigma around being in a same-sex couple, were less likely to report experiencing (OR 0.91, 95%CI 0.85, 0.99) or perpetrating sexual violence (OR 0.90, 95%CI 0.83, 0.98). Conversely, men who scored high on the perceived local stigma-individual scale, and thus reported a perception of more stigma around being a gay/bisexual man, were more likely to report experiencing physical violence (OR1.03, 95%CI 1.00, 1.07).
DISCUSSION
From the relatively small number of studies that have examined IPV in male same-sex relationships, the rates of male-to-male IPV range between 11% and 44%.29 This variability reflects different definitions of partner abuse across studies and makes cross-study comparisons very difficult. Few studies have examined multiple forms of IPV, with most focusing on one specific form of violence in isolation. The majority of studies have focused on sexual or physical violence, with a dearth of studies that have examined emotional IPV among MSM. The results presented here find slightly lower levels of both physical and sexual IPV than have been shown in some previous studies, yet show relatively high levels of reporting of the experience of emotional IPV, which has often been overlooked in previous studies of IPV in same-sex relationships. Of particular surprise here are the high levels of reporting of perpetration of IPV, with over one-third of men reporting that they have perpetrated emotional violence against a partner, one-fifth reporting perpetrating physical violence and nine percent reporting perpetration of sexual violence.
Previous studies of IPV among gay and bisexual men, using a similar method of recruiting participants for a survey via ads placed on social network sites, found less than four percent of men reported perpetrating physical violence and less than one percent reported perpetrating sexual violence.30 The difference between the two studies lies in differences in how experiencing or perpetrating violence was measured. In the current study, we used the Conflict Tactics Scale Revised, which uses multiple questions for each type of violence. 28 For example, to measure physical violence, participants were asked if they had experienced/ perpetrated kicking, shoving, being beaten-up etc. However, in the previous study, which produced much lower rates of perpetration of IPV, participants were asked a single question for each type of violence, for example “has your partner ever tried to hurt you, this includes pushing, holding you down, hitting you with his fist, kicking, attempting to strangle, attacking with a knife, gun or other weapon?” Covering a range of behaviors that constitute emotional, physical and sexual violence is more sensitive in capturing the reporting of both the experience and perpetration of violence among MSM.
Many previous studies have relied on convenience samples of clinic-based populations. The recruitment of LGBT individuals into studies of IPV has posed a challenge to researchers, due primarily to perceived difficulties in disclosing sexual orientation; as such, many previous studies have used convenience samples recruited through LGBT venues and publications.7 The results presented here demonstrate the feasibility of collecting IPV data through surveys administered through social networking sites, providing a new opportunity to reach currently overlooked populations in IPV research. A significant contribution of this work is in the demonstration of the feasibility of using internet-based surveys to collect IPV data from marginalized groups in the U.S. The study was completed relatively quickly and inexpensively using a methodology that can be implemented in future research to gather data from hard-to- reach population groups on a range of topics. Data are often needed to inform new policy directions that may impact understudied and potentially marginalized groups for which researchers and policymakers have little available information.
The factors significantly associated with the reporting of IPV point to the role of minority stress in shaping the risk of experience or perpetration of violence. MSM respondents with lower levels of education, who identified as a racial minority, or who self-reported as HIV-positive, were all more likely to report increased experience or perpetration of IPV. Lower levels of education may be associated with lower levels of income and a lack of access to social capital and resources, and thus creating an economic stress that manifests as perpetration of or vulnerability to IPV. MSM who identify as a racial minority may face stress through exposure to racism, both in the MSM community and beyond, or through increased levels of homophobia known to exist in communities of color in the U.S.31,32 However, the sample for this study was predominantly white, with too few numbers in each of the ethnic and racial groups to allow a deeper investigation other than white versus other of the racial differences in IPV among MSM. Finally, MSM who identify as HIV-positive may experience stress through living with HIV, the need for consistent access to care, or through discrimination arising from the stigma often associated with being HIV-positive. This may explain the finding that HIV-positive men are more likely to report perpetrating physical violence. Heintz and Melendez33 report that gay men in abusive relationships are at a greater risk of HIV infection due to a lack of ability to negotiate for safer sex with their partner, and through coerced sexual activity. The result found here, that HIV-positive MSM are more likely to report experiencing sexual violence, may reflect the unsafe sexual activities experienced by MSM in abusive relationships, and the resultant increased risk of HIV infection. This finding also has important policy implications for efforts that seek to reduce spread of HIV and other sexually transmitted infections in hard to reach populations.
Interestingly, MSM who perceived more stigma to being in a male same-sex couple were less likely to report sexual violence. MSM who perceive their relationship to be stigmatized may be less likely to report sexual violence due to a perceived lack of resources or support. Unique to this study is the inclusion of scales to measure dyadic characteristics in the modeling of IPV. MSM who reported greater satisfaction with their relationship were less likely to report violence, which although not surprising, points to the fact that MSM see a satisfying relationship as one that does not include violence. MSM who reported a higher degree of concordance with their partner on lifestyle choices were also less likely to report violence: again, this shows the role of stress in creating the risk of IPV. Couples who disagree on lifestyle choices may face stress through arguments that lead to violence: alternatively, the experience of violence may reduce the ability of one member of the couple to negotiate for and agree upon concordance around lifestyle choices. These results largely mirror the dyadic model of partner violence (Bartholomew and Cobb26), which states that couples in more mutually satisfying relationships, with high levels of trust and strong communication, are less likely to experience IPV. A second contribution of this research is the demonstration that dyadic models of IPV originally developed for heterosexual couples may be equally applicable to same-sex couples. This finding also underscores the need for policy and legislative initiatives to more deliberately include experiences of sexual minorities, in particular, same-sex couples.
LIMITATIONS
The key limitations to the present results are a small sample size and possible selection bias in both the decision to complete the questionnaire and the decision to answer the questions on IPV. Kaschak12 refers to the “double closet” that surrounds IPV in same-sex relationships; the dual burden of shame and silence surrounding both the discussion of IPV and the discussion of sexuality, hence it is possible that IPV may be under-reported. Additionally, the cross-sectional nature of the data means that only associations between dyadic characteristics and the reporting of IPV can be drawn; there are no causal relationships identified here. In many of the associations identified the relationship could work two ways: for example, HIV-positive status could lead to IPV, or IPV could lead to HIV infection. Further work, using longitudinal data, is required to further understand the relationships between dyadic characteristics and IPV among MSM.
CONCLUSION
The results presented here demonstrate high levels of IPV among MSM, and illustrate how an online survey coupled with social networking sites can be used to collect data on sensitive public health issues such as IPV for marginalized groups such as MSM. The results also demonstrate similarities in the dyadic factors shaping IPV in heterosexual and homosexual relationships, an area that has been largely overlooked in the existing literature. There is clearly a need for further research into issues surrounding IPV in same-sex male relationships, who are a population vulnerable to high levels of IPV, and to understand the complex relationships that exist between IPV and dyadic characteristics. Such information is vital for the development of effective interventions to reduce IPV and improve health, in particular sexual health, among MSM in the U.S. The results presented here may help to inform the development of IPV screening tools for MSM, and add to the creation of more sensitized and culturally appropriate prevention messages aimed at MSM couples, who have to date been largely missing from prevention efforts.
Footnotes
This work was supported by a grant from the National Institutes of Mental Health, R34-MH086331. The authors thank Russell Tarver for his assistance with programming and administering the online survey.
Supervising Section Editor: Monica H. Swahn, PhD, MPH
Submission history: Submitted: January 19, 2011; Revision received March 2, 2011; Accepted March 3, 2011.
Reprints available through open access at http://escholarship.org/uc/uciem_westjem.
Address for Correspondence: Rob Stephenson, PhD
Hubert Department of Global Health, Rollins School of Public Health, 1518 Clifton Rd., Atlanta, GA, 30322
Email: rbsteph@sph.emory.edu
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. McClennen JC, Summers B, Vaugh C. Gay men’s domestic violence: dynamics, help-seeking behaviors, and correlates. J of Gay and Lesbian Social Services. 2002;14(1):23–49.
2. McClennen JC. Domestic violence between same-gender partners recent findings and future research. J of Interpersonal Violence. 2005;20(2):149–154.
3. Gay Demographics Census information on gay and lesbian couples. 2000. Available athttp://www.gaydemographics.org. Last accessed October 17, 2006,
4. Pope M, Barrel B. Counseling gay men toward an integrated sexuality. In: Burlew LD, Capuzzi D, editors. Sexuality counseling. Hauppague, NY: Nova Science; 2002. pp. 149–75.
5. Aulivola M. Outing domestic violence: Affording appropriate protections to gay and lesbian victims. Family Court Review. 2004;42:162–77.
6. Barnes PG. It’s just a quarrel. J of the Am Bar Asso. 1998;84:24–5.
7. Balsam KF, Fothblum ED, Beauchaine TP. Victimization over the life span: a comparison of lesbian, gay, bisexual, and heterosexual siblings. J of Consulting and Clinical Psych. 2005;74(3):477–87.
8. Halpern CT, Young ML, Waller MW, et al. Prevalence of partner violence in same-sex romantic and sexual relationships in a national sample of adolescents. J of Adolescent Health. 2004;35:124–31.
9. Burke TW, Jordan ML, Owen SS. A cross-national comparison of gay and lesbian domestic violence. J of Contemporary Criminal Justice. 2002;18:231–56.
10. Alexander CJ. Violence in gay and lesbian relationships. J of Gay and Lesbian Social Services.2002;14(1):95–8.
11. Browning C. Silence on same-sex partner abuse. Alternate Routes. 1995;12:95–106.
12. Kaschak E. Intimate betrayal: domestic violence in lesbian relationship. Women and Therapy.2001;23(3):1–5.
13. Peterman LM, Dixon CG. Domestic violence between same-sex partners: Implications for counseling. J of Counseling and Dev. 2003;81(1):40–7.
14. Pitts EL. Domestic violence in gay and lesbian relationships. Gay and Lesbian Med Associa Jl.2000;4:195–6.
15. National Center on Domestic and Sexual Violence Lesbian/gay power and control wheel.(adapted from Domestic Abuse Intervention Project, Duluth, MN). National Center on Domestic and Sexual Violence. Available at http://www.ncdsv.org/publication_wheel.html. Last accessed March 28, 2006.
16. Elliott P. Shattering illusions: Same-sex domestic violence. J of Gay and Lesbian Social Services.1996;4(1):1–8.
17. De Vidas M. Childhood sexual abuse and domestic violence: A support group for Latino gay men and lesbians. Journal of Gay and Lesbian Social Services. 1999;10(2):51–68.
18. Greenwood GL, Relf MV, Huang B, et al. Battering victimization among a probability-based sample of men who have sex with men. Am J of Public Health. 2002;92:1964–9. [PMC free article][PubMed]
19. Waldner-Haugrud LK, Gratch LV, Magruder B. Victimization and perpetration rates of violence in gay and lesbian relationships: Gender issues explored. Violence and Victims. 1997;12(2):173–84.[PubMed]
20. Toro-Alfonso J, Rodriguez-Madera S. Sexual coercion in a sample of Puerto Rican gay males. J of Gay & Lesbian Social Services. 2004;17:47–58.
21. Cruz JM. ‘Why doesn’t he just leave?’: gay male domestic violence and the reasons victims stay. J of Men’s Studies. 2003;11(3):309–23.
22. Cruz JM, Firestone JM. Exploring violence and abuse in gay male relationships. Violence and Victims. 1998;13(2):159–73. [PubMed]
23. Cruz JM, Peralta RL. Family violence and substance use: The perceived effects of substance use within gay male relationships. Violence and Victims. 2001;16:161–72. [PubMed]
24. Blosnich JR. Violence by any other name: Using population-based data to explore intimate partner violence (IPV) among same-sex relationships in the United States. 2008.
25. Potoczniak MJ, Mourot JE, Crosbie-Burnett M, et al. Legal and psychological perspectives on same-sex domestic violence: A multi-systemic approach. J of Family Psychology. 2003;17:252–9.
26. Bartholomew K, Cobb RJ. Conceptualizing Relationship Violence as a Dyadic Process. In: Horowitz LM, Strack S, editors. Handbook of Interpersonal Psychology: Theory, Research, Assessment and Therapeutic Interventions. John Wiley & Sons, Inc; Hoboken, New Jersey: 2010. pp. 233–47.
27. Lewis MA, McBride CM, Pollak KI, et al. Understanding health behavior change among couples: an interdependence and communal coping approach. Social Science and Medicine.2006;62(6):1369–80. [PubMed]
28. Straus MA. Measuring Intrafamily Conflict and Violence: The Conflict Tactics (CT) Scales. J of Marriage and Family. 1979;41:175–88.
29. Herek GM, Sims C. Sexual orientation and violent victimization: Hate crimes and intimate partner violence among gay and bisexual males in the United States. In: Wolitski RJ, Stall R, Valdiserri RO, editors. Unequal opportunity: Health disparities among gay and bisexual men in the United States.New York: Oxford University Press; 2008. pp. 35–71.
30. Stephenson R, Khosropour C, Sullivan PS. Reporting of intimate partner violence among men who have sex with men in an on-line survey. West J of Emerg Med. 2010;11(3):242–6.[PMC free article] [PubMed]
31. Adams CL, Kimmel DC. Exploring the lives of older African American gay men. In: Greene B, editor. Ethnic and cultural diversity among lesbian and gay men. Thousand Oaks, Inc CA: Sage Publications, Inc; 1997. pp. 132–51.
32. Savin-Williams RC. Verbal and physical abuse as stressors in the lives of lesbian, gay male, and bisexual youths: Associations with school problems, running away, substance abuse, prostitution, and suicide. J of Consulting and Clinical Psychology. 1994;62:261–9.
33. Heintz AJ, Melendez RM. Intimate partner violence and HIV/STD risk among lesbian, gay, bisexual, and transgender individuals. J of Interpersonal Violence. 2006;21(2):193–208.