
{kind=link}
| Author | Affiliation |
|---|---|
| Terry Kowalenko, MD | University of Michigan, Department of Emergency Medicine, Ann Arbor, Michigan |
| Samantha R. Hauff, MD | University of Michigan, Department of Emergency Medicine, Ann Arbor, Michigan |
| Peter C. Morden, MD, MPH | Wayne State University, Detroit, Michigan |
| Barbara Smith, BA | University of Michigan, Department of Emergency Medicine, Ann Arbor, Michigan |
ABSTRACT
Introduction:
Healthcare and social workers have the highest incidence of workplace violence of any industry. Assaults toward healthcare workers account for nearly half of all nonfatal injuries from occupational violence. Our goal was to develop and evaluate an instrument for prospective collection of data relevant to emergency department (ED) violence against healthcare workers.
Methods:
Participants at a high-volume tertiary care center were shown 11 vignettes portraying verbal and physical assaults and responded to a survey developed by the research team and piloted by ED personnel addressing the type and severity of violence portrayed. Demographic and employment groups were compared using the independent-samples Mann-Whitney U Test.
Results:
There were 193 participants (91 male). We found few statistical differences when comparing occupational and gender groups. Males assigned higher severity scores to acts of verbal violence versus females (mean M,F=3.08, 2.70; p<0.001). While not achieving statistical significance, subgroup analysis revealed that attending physicians rated acts of verbal violence higher than resident physicians, and nurses assigned higher severity scores to acts of sexual, verbal, and physical violence versus their physician counterparts.
Conclusion:
This survey instrument is the first tool shown to be accurate and reliable in characterizing acts of violence in the ED across all demographic and employment groups using filmed vignettes of violent acts. Gender and occupation of ED workers does not appear to play a significant role in perception of severity workplace violence.
INTRODUCTION
Violence in the healthcare setting is not uncommon, and the emergency department (ED) has the highest rate of violence in the hospital.1 In 2004 the Bureau of Labor Statistics released data collected from 1996–2000, reporting that nearly half of all acts of workplace violence occur in healthcare settings.2 While often thought to be a phenomenon encountered primarily in large urban EDs, violent acts occur regardless of practice size and setting.3 Many acts of violence towards staff go unreported as they are considered “part of the job.” The ED is unique among healthcare settings in that it serves a higher proportion of patients suffering from substance abuse and psychiatric illness. EDs are frequently chaotic, crowded, and understaffed. Patients often wait hours for care and frequently occupy hallway beds, both of which can lead to frustration. Not infrequently, patients and their visitors carry weapons.4
Workplace violence influences job performance, retention, and stress.5–7 Gates et al found that in the ED 25% of nurses seldom or never felt safe at work, and that there was a significant inverse relationship between feeling safe and job satisfaction.7 This was supported by Kansagra et al6 in a survey of 65 EDs that showed 25% of staff across all occupational groups felt safe sometimes, rarely, or never. Victims also experience more permanent scars as 1 study found that over one-third suffered psychological problems following assault.8
Kowalenko et al surveyed Michigan emergency physicians and showed that over a 1 year period 75% were threatened verbally and 28% were physically assaulted.9 Multiple survey-based studies have confirmed these high rates of violence against ED healthcare workers in the United States and internationally.1,3–11
Review of the literature reveals there are no studies that describe a validated tool or survey instrument that may be used to prospectively evaluate violence in the ED. Much of the literature relies on survey data and the bulk focuses on violence towards a single occupational group.1,3,5–10 Additionally, most studies define violent acts as physical acts, neglecting the importance of verbal threats.
The purpose of this pilot study was to develop and evaluate a survey instrument (Figure 1) for prospective collection of data relevant to ED violence and to document ED personnel’s perception of aggressive patient encounters based on filmed vignettes. This tool will enable investigation into environmental and behavioral factors surrounding violence against ED healthcare workers and may be used to potentially develop effective interventions to decrease the incidence and severity.
METHODS
All ED personnel employed at the time of the study initiation (April, 2008) at a large, tertiary care hospital were eligible. This study was specifically designed to incorporate all ED workers to assure that the survey instrument consistently and accurately captured the appropriate violent act regardless of gender or job title. Participants viewed 11 vignettes on-line or via DVD depicting acts of physical, sexual, and verbal violence of varying degrees of severity, and completed the survey instrument (Figure 1). They then rated the severity of the incident on a scale from 1–6, with 1 being “least” severe and 6 being the “most” severe. Participants were asked to use the following definitions when answering the survey questions about the vignettes:
-
Physical assaults include hitting with body part, slapping, kicking, punching, pinching, scratching, biting, pulling hair, hitting with an object, throwing an object, spitting, beating, shooting, stabbing, squeezing, and twisting.
-
Physical threats include actions, statements, written or non-verbal messages conveying threats of physical injury which were serious enough to unsettle your mind. It includes expressions of intent to inflict pain, injury, or punishment.
-
Verbal harassment includes cursing, cussing, yelling at or berating a person in front of another, racial slurs, or humiliating and patronizing actions.
-
Sexual harassment includes unwelcome sexual advances, requests for sexual favors, and other verbal or physical conduct of a sexual nature, insulting gestures, whistling, jokes or humor about gender specific traits, offensive pictures, and offensive contact, such as patting, pinching, brushing against body, attempting or actual fondling, or kissing.
These definitions have been used in other studies to identify physical, verbal, and sexual assaults.12 Participants were also informed that complaining and profanity alone without an imbedded threat, should not be considered a violent act.
Participants were over 18 years of age, and recruited via workplace e-mail. This study was approved by the University of Michigan Institutional Review Board.
We adapted the survey instrument from the questionnaire used by Kowalenko, et al,9which was originally designed to capture violent acts perpetrated against attending physicians in a retrospective manner and had many questions geared toward determining resources available, who was the perpetrator, and the physician’s response to the acts. This study also looked at encounters outside the ED and incidents of stalking, neither of which were necessary in the current study’s questionnaire given the real-time nature of the vignettes. The survey questions extracted from the Kowalenko et al9 study were those that focused on demographics and the specific type of violent act. The instrument was further revised by members of the research team to ensure question clarity. It was then sent to an independent group of ED personnel, including an attending, resident, and nurses for suggestions and or revisions. The tool and vignettes were then piloted by several personnel prior to initiation of the study. Although these differences did not reach statistical significance.
The vignettes were based on actual reported violent encounters in the ED and scripted by an experienced emergency physician well-versed in healthcare workplace violence. These vignettes represented a broad range of violent incidents which commonly occur in EDs. These were reviewed and edited by a small group of ED personnel that included physicians (attending and resident), a nurse, a medical student, and a research coordinator. Using the aforementioned definitions of violent acts as a guideline, this group collectively reached consensus apriori determining the type and intended level of violence perpetrated prior to the surveys and vignettes being sent to participants. To avoid biasing viewers’ responses due to personal relationships, the vignette actors were volunteers who did not work in the ED. The vignettes consisted of an incident portraying an angry patient who does not specifically threaten harm, 3 situations in which a verbal threat is made to a healthcare provider, 5 physical assault incidents of varying severity, and 2 portrayals of sexual assault involving inappropriate touching (1 victim was male, the other female). Respondents were asked to provide comments regarding the tool after completion of the survey.
We performed descriptive statistics and comparisons using PAWS Statistic 18 – SPSS (IBM, 2010). The differences between demographic and employment sub-group’s severity rating of each vignette was examined using the independent-samples Mann-Whitney U test, stratified by gender and occupation. All tests of statistical significance were set at a predetermined level of 0.05.
RESULTS
There were 193 participants, (91 male, 89 female, and 13 who declined to provide a gender identifier). This included 42 attending physicians, 28 residents, 3 mid-level providers, 32 nurses, 18 technicians, 36 security officers, 15 social workers, and 12 clerks. The majority of respondents worked in the adult ED (n=143, 76.9%). However, a substantial proportion (n=75, 40.3%) worked in the pediatric ED and in the psychiatric ED (n=66, 35.5%). Most worked in more than one setting, therefore the percentages are greater than 100%.
Occupational and gender groups overall had very similar perceptions of sexual, verbal and physical acts of violence in the ED (Table 1). Males perceived acts of verbal violence to be more severe than their female co-workers (mean M, F=3.08, 2.70; p<0.001).
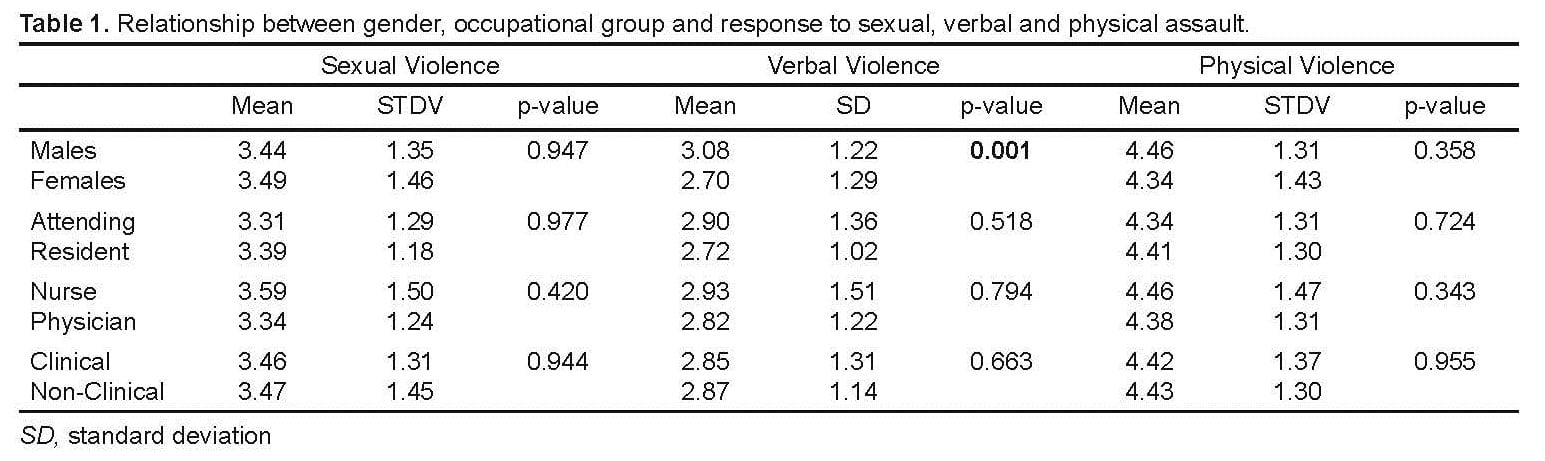
Relationship between gender, occupational group and response to sexual, verbal and physical assault.
There were no differences between any groups with regard to severity scores of sexual or physical violence. There were no statistically significant differences between nurses and physicians, nor clinical and non-clinical workers in the response to depictions of sexual, verbal, or physical violence (Table 1).
To look at subtle differences between gender and occupational groups, post hoc analysis was performed examining violence severity ratings grouping them into “Low” severity (scores of 1–2), “Medium” severity (scores of 3–4), and “High” severity (scores of 5–6) (Table 2). This revealed that attending physicians rated acts of verbal violence higher than resident physicians, and nurses assigned higher severity scores to acts of sexual, verbal, and physical violence versus their physician counterparts.
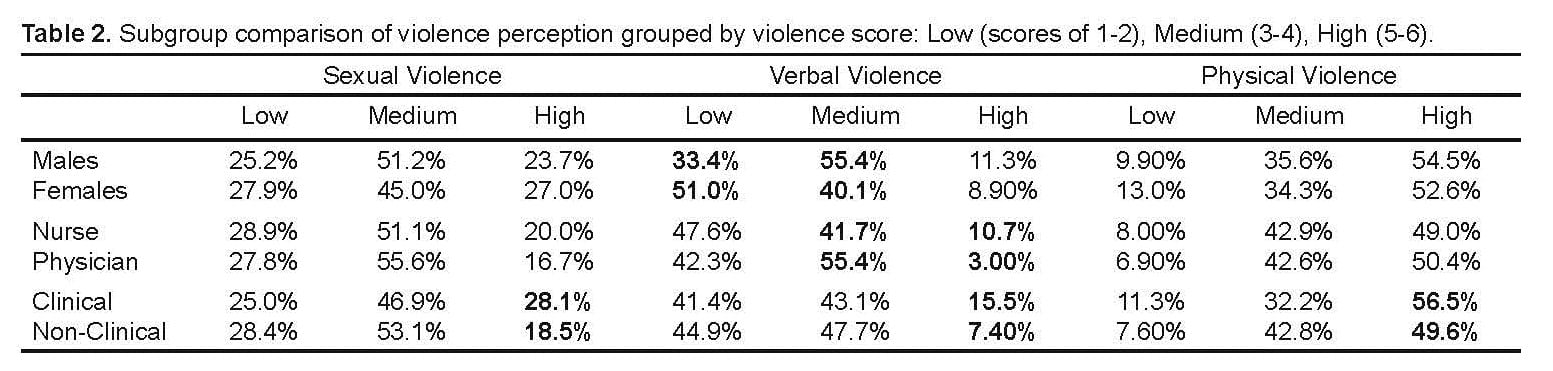
Subgroup comparison of violence perception grouped by violence score: Low (scores of 1–2), Medium (3–4), High (5–6).
The only consistent comment regarding the study was that it took participants a long time to complete 11 vignettes; however, there were no specific comments or concerns regarding the survey instrument itself.
DISCUSSION
Many previous studies have reported on the incidence and reaction to violence against healthcare workers; however, none have specifically looked at the data collection tool. Most of these studies have been performed in a retrospective manner. As a result of the retrospective nature of the data collection, it is subject to personal recall bias and it is unclear if any 2 individuals perceived the violent act the same way. Having a tool that accurately captures the violent act is important for future epidemiologic and prevention studies. To our knowledge no one has had multiple healthcare workers independently view the same violent act, then report on it using a single survey instrument. This pilot study was intended to create a survey tool that would accurately capture violent severe acts perpetrated against healthcare workers in real time.
In our study multiple different ED healthcare workers viewed vignettes of a broad range of violent acts commonly seen in the ED and reported on what they saw using a single survey instrument. The vignettes were designed and agreed upon by the research team along with several other healthcare workers apriori to depict several different verbal, physical and sexual assaults.
While it may be anticipated that non-clinical workers and those who work primarily in a pediatric setting may be less accustomed to acts of physical violence and therefore assign higher severity scores, this was not the case. Males assigned higher severity scores than females to acts of verbal violence. This appeared somewhat counter intuitive. This may be due to males generally experiencing more acts of violence, thereby causing them to be more sensitized and have a lower tolerance threshold. An alternative explanation is that females want to appear, or just are, less disturbed by threats because they have become so accustomed to the frequency of events. That nurses gave higher severity scores than physicians for all subtypes of violence is not surprising given that nurses are on the “front line” of patient care and more frequently experience physical violence.7, 10
While not statistically significant, differences were found between attending and resident physician responses with regard to verbal threats, as attendings assigned higher severity scores. This may be due to the resident’s perception of having to “perform” for both their attendings, as well as the patients. They cannot appear to be upset by this affront in the eyes of those evaluating them. In addition, residents frequently spend proportionally more time with patients and therefore are more likely to be exposed to verbal threats. This may help them become more accustomed or tolerant.
Consideration should be given to the setting and study population. Healthcare workers who self-select for ED employment may be more accustomed to coping with workplace violence than those in other clinical settings. Application of this tool should be expanded to incorporate the perceptions of workers hospital-wide.
To collect meaningful data that characterize violence in the ED (and potentially other healthcare settings) a validated tool is needed. The lack of variability between respondents in the ED suggests this is a reliable tool to characterize healthcare workers’ response to violence in the workplace. The specific aims of this study were to create a reliable instrument that consistently and accurately captured data regarding the actual violent or threatening acts regardless of who saw or experienced the event. This tool has achieved these goals.
LIMITATIONS
Of the eligible participants, 55% completed the survey instrument for all 11 vignettes. It is unclear if those who did not participate would have answered differently. However, the respondents made up a representative sample of ED personnel and it is unlikely that a greater response rate would have resulted in different findings.
Given the lack of variation between gender and occupational groups with regard to severity score, it is unlikely that a correction coefficient would be necessary in applying this tool.
Additionally, this tool was assessed in a single, tertiary care academic ED. It is unclear whether responses would be different in other settings. Filmed vignettes may not illicit the same emotional response as when an individual is an actual victim to a violent incident, thereby resulting in lower response scores.
CONCLUSION
The survey instrument used in this pilot study is the first tool to be used in characterizing acts of violence using filmed vignettes across demographic and employment groups. This tool should be employed and evaluated in actual ED settings to confirm its validity. This tool has the potential to assist in data collection for the prospective evaluation of ED violence. Gender and occupation of ED workers does not appear to play a significant role in perception of severity workplace violence. The authors intend to use this tool in a prospective study to examine both verbal and physical violence in the ED to better define this widespread problem. This tool will enable further investigation into environmental and behavioral factors that can be used in the development of effective interventions that may decrease the incidence and severity of violence against healthcare workers.
Footnotes
Supervising Section Editor: Larry Raney, MD
Submission history: Submitted May 12, 2011; Revision received August 12, 2011; Accepted December 5, 2011
Full text available through open access at http://escholarship.org/uc/uciem_westjem
DOI: 10.5811/westjem.2011.12.6795
Address for Correspondence: Terry Kowalenko, MD, University of Michigan, 1500 E. Medical Center Dr. SPC 5305 Ann Arbor, MMI 48100-5305
Email: terryk@med.umich.edu
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Stultz MS. Crime in hospitals 1995: the latest International Association for Healthcare Security and Safety Survey. J Healthc Prot Manage. 1996–1997 13-1-45.
2. Guidelines for preventing workplace violence for health care and social service workers. Occupational Safety and Health Administration website. Available at:www.osha.gov/publications/osha3148.pdf. Accessed 8 September 2009.
3. Blando JD, McGreevy K, O’Hagan E, et al. Emergency Department Security Programs, Community Crime, and Employee Assaults. J Emerg Med. doi: 10.1016/j.jemermed.2008.06.026. Epub ahead of print Jan 2, 2009; [Cross Ref]
4. Ordog GJ, Wasserberger J, Ordog C, et al. Weapon carriage among major trauma victims in the emergency department. Acad Emerg Med. 1995;2(2):109–13. [PubMed]
5. Fernandes CMB, Bouthillette F, Raboud JM, et al. Violence in the emergency department: a survey of health care workers. CMAJ. 1999;161(10):1245–1248.[PMC free article] [PubMed]
6. Kansagra SM, Rao SR, Sullivan AF, et al. A Survey of Workplace Violence Across 65 U.S. Emergency Departments. Acad Emerg Med. 2008;15(12):1268–1274.[PMC free article] [PubMed]
7. Gates DM, Ross CS, McQueen L. Violence against emergency department workers. J Emerg Med. 2006;31(3):331–337. [PubMed]
8. Boz B, Acar K, Ergin A, et al. Violence Toward Health Care Workers in Emergency Departments in Denizli, Turkey. Adv Ther. 2006;23(2):364–369. [PubMed]
9. Kowalenko T, Walters BL, Khare RK, et al. Workplace Violence: A Survey of Emergency Physicians in the State of Michigan. Annals Emerg Med. 2005;46(2):142–147.
10. Gacki-Smith J, Juarez AM, Boyett L, et al. Violence against nurses working in US emergency departments. J Nurs Adm. 2009;39(7–8):340–349. [PubMed]
11. Carmi-Iluz T, Peleg R, Freud T, et al. Verbal and physical violence towards hospital and community-based physicians in the Negev: An Observational Study. BMC Health Serv Res. 2005;5:54–59. [PMC free article] [PubMed]
12. Gates D, Kowalenko T, Gillespie G, et al. Occupational and Demographic Factors Associated with Violence in the Emergency Department. Accepted for publication: Advanced Emergency Nursing Journal – AENJ-D-11-00007.