
{kind=link}
| Author | Affiliation |
|---|---|
| Scott M. Sasser, MD | Emory University School of Medicine, Department of Emergency Medicine, Atlanta, GA |
| Eric Ossmann, MD | Duke University School of Medicine, Department of Emergency Medicine, Durham, NC |
| Marlena M. Wald, MPH, MLS | Centers for Disease Control and Prevention, Division of Injury Response, Atlanta, GA |
| E. Brooke Lerner, PhD | Medical College of Wisconsin, Department of Emergency Medicine, Milwaukee, WI |
| Richard C. Hunt, MD | Centers for Disease Control and Prevention, Division of Injury Response, Atlanta, GA |
ABSTRACT
Introduction:
When emergency medical services (EMS) providers respond to the scene of an injury, they must decide where to transport the injured patients for further evaluation and treatment. This is done through a process known as “field triage”, whereby a patient’s injuries are matched to the most appropriate hospital. In 2005–2006 the National Expert Panel on Field Triage, convened by the Centers for Disease Control and Prevention and the National Highway Traffic Safety Administration, revised the 1999 American College of Surgeons Committee on Trauma Field Triage Decision Scheme. This revision, the 2006 Field Triage Decision Scheme, was published in 2006.
Methods:
State Public Health departments’ and EMS’ external websites were evaluated to ascertain the current status of implementation of the 2006 Field Triage Decision Scheme.
Results:
Information regarding field triage was located for 41 states. In nine states no information regarding field triage was available on their websites. Of the 41 states where information was located, seven were classified as “full adopters” of the 2006 Field Triage Decision Scheme; nine were considered “partial adopters”; 17 states were found to be using a full version or modification of the 1999 Field Triage Decision Scheme; and eight states were considered to be using a different protocol or scheme for field triage.
Conclusion:
Many states have adopted the 2006 Decision Scheme (full or partial). Further investigation is needed to determine the reasons why some states do not adopt the guidelines.
INTRODUCTION
In the United States (U.S.), injury is the leading cause of death for persons aged 1–44 years.1 In 2007, injuries were responsible for approximately 182,000 deaths in the U.S.,1 with an additional 25 million injuries serious enough to require a hospital emergency department (ED) visit.2 When an injury does occur and emergency medical services (EMS) providers respond, they must decide where to transport the injured patients for further evaluation and treatment. This is done through a process known as “field triage,” whereby a patient’s injuries are matched to the most appropriate hospital. The destination hospital (trauma center or a nontrauma center) chosen by the EMS providers has been shown to have an impact on an individual patient’s outcome. The National Study on the Costs and Outcomes of Trauma reported a 25% reduction in mortality for severely injured patients who received care at a Level I trauma center rather than at a nontrauma center.3
In order to assist with destination transport decisions, EMS providers and their medical directors use field triage decision schemes to help ensure that they get the right person, to the right place, at the right time. These schemes are typically a combination of physiologic, anatomic, and mechanistic criteria that are intended to identify those patients with, or at risk of, a severe injury. Instead of developing individual decision schemes de novo, many states and local communities have used a version promulgated by the American College of Surgeons-Committee on Trauma (ACS-COT). This scheme was first published in 1986.4 It grew out of early efforts of the ACS-COT to develop a resource monograph that would provide guidance for the designation of certain healthcare facilities as trauma centers and for the care of the acutely injured.5 Between 1986 and 1999, the ACS-COT Decision Scheme was revised three times (1990, 1993 and 1999).6–8 With each revision, the scheme was re-evaluated by the ACS-COT and analyzed in the context of the available literature and expert opinion. Recommendations were then developed regarding modifications to the scheme.
In 2005, the National Expert Panel on Field Triage was established to guide the 2006 revision of the field triage scheme. This group was formed by the Centers for Disease Control and Prevention (CDC) in collaboration with ACS-COT and the National Highway Traffic Safety Administration (NHTSA). The group sought to bring additional disciplines into the revision process (e.g., emergency medicine, EMS, public health, the automotive industry and additional federal agencies). The goals of the panel were to provide a thorough review of the 1999 field triage scheme, examine and consider new and existing evidence, and assist with the dissemination and implementation of any revisions. The 2006 Field Triage Decision Scheme (Figure 1) was published by the ACS-COT in 2006 and was subsequently endorsed by 17 national organizations representing the spectrum of public health and acute injury care, with concurrence from NHTSA.9–10 A description of the process of revision and the detailed rationale behind deleted, modified, and new triage criteria in the scheme was published in the CDCMorbidity and Mortality Weekly Report (MMWR) Recommendations and Reports in January 2009.10
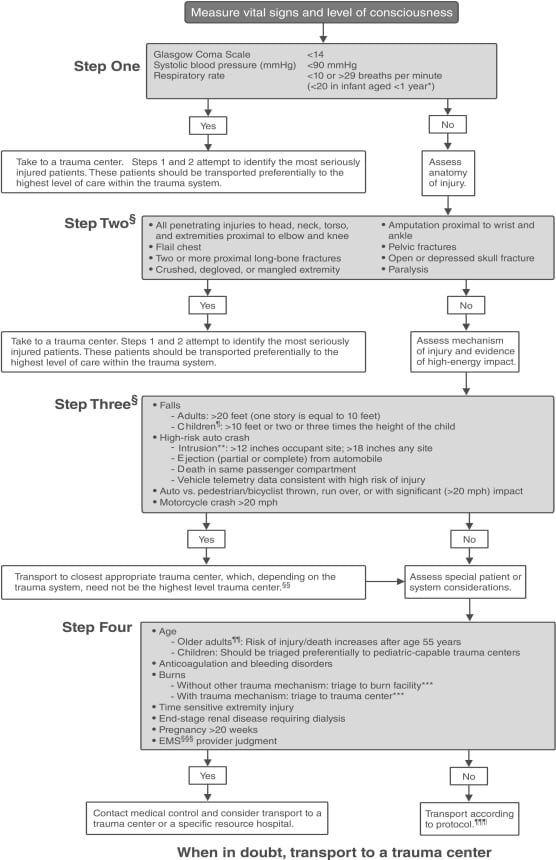
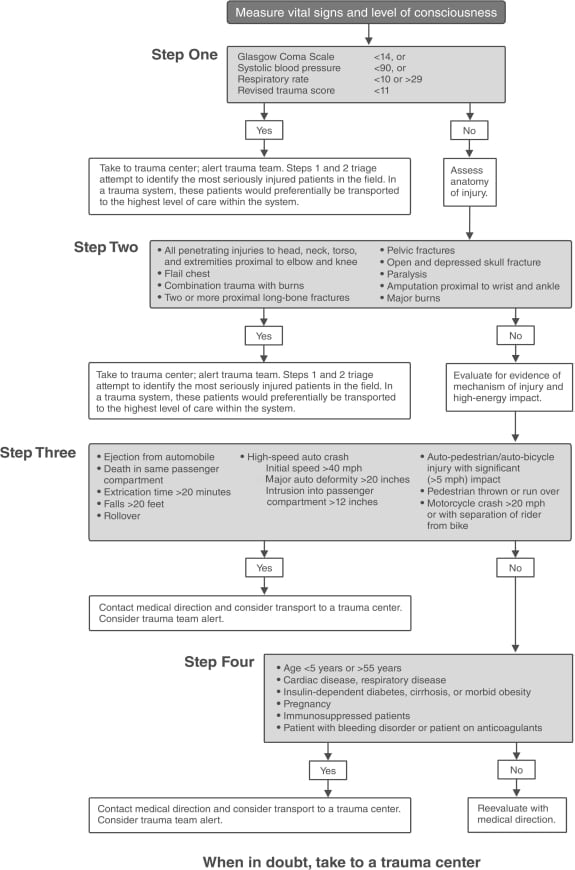
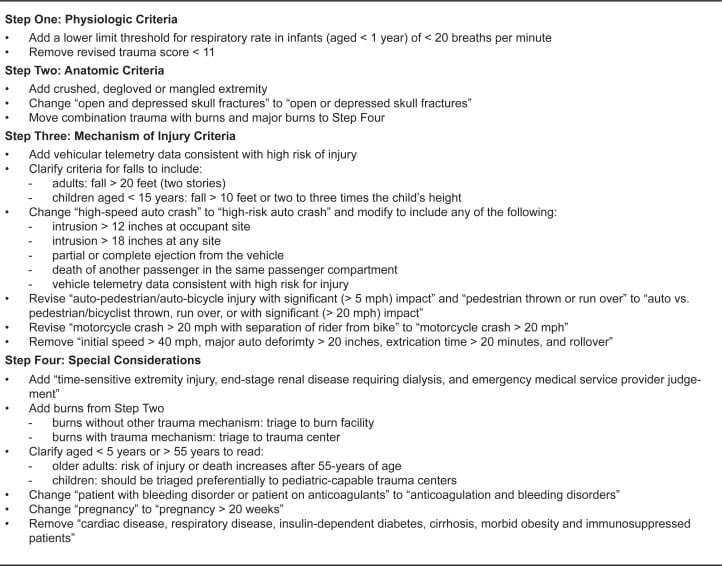
The 2006 Field Triage Decision Scheme contains several important changes from the 1999 scheme (Figure 2) and these specific changes are outlined in Figure 3. Following the release of the 2006 Field Triage Decision Scheme, multiple efforts have been underway to disseminate the scheme and the rationale for the revision process contained within the MMWR.10 Our study was conducted to gauge the implementation and use of the 2006 Field Triage Decision Scheme in the U.S. The objective of this study was to determine how many states have public documents demonstrating that they have adopted the 2006 Field Triage Guideline into their EMS protocols, using readily available public information and resources.
Since the expansion of online connectivity among the general public, websites for scientific and governmental information in the U.S. have developed to include comprehensive federal, state, county and municipal sites. Using simple search heuristics, internet search engines such as Google™, Yahoo™ and Bing™, has allowed the public and specialists alike ease of access to laws, policies and other administrative materials once difficult to locate and obtain in print.11 The use of publicly available websites for this study was appropriate because we hypothesize that the presence of the guidelines on an individual state’s website is a proxy for state adoption of the 2006 guideline.
METHODS
This project used online search engines to examine publicly available state EMS and health departments’ websites. Searches were conducted during October 1, 2009, through April 30, 2010. The search engine Google™ was selected because of its volume of searches, with an average in the U.S. of six billion searches per month.12 The authors inferred that a person searching for this type of information would likely use this search engine. For each state, authors used search terms such as field triage, trauma, triage guidelines, triage protocols, prehospital injury triage, and others. Authors examined websites for existing EMS protocols, memorandums, committee notes, and legislative or regulatory language. Once evidence of full or partial adoption was found, authors downloaded the relevant materials for each state .Two board certified and EMS fellowship trained emergency physicians (authors SMS and EO) independently examined the information. The reviewers carefully examined these materials with comparison to the 2006 Field Triage Decision Scheme and prior ACS-COT guidelines to ascertain the level of adoption (full or partial) by each governmental unit. If the reviewers agreed, the findings were entered into the database. If there was disagreement, the findings were discussed. If no consensus was reached, a third reviewer (EBL) was asked to examine the material to make a final determination. If no information was available on the publicly available websites, the state was documented as “information not available.”
We considered a given state to have “full adoption” if the 2006 Decision Scheme was reproduced in its entirety on the website without modifications or if state legislation, rules, or committee minutes made direct reference to use of recommendations for the 2006 Decision Scheme. We considered states with only minor, non-substantial, additions (e.g., additional vital sign, or a language edit) to the complete 2006 Decision Scheme to be full adopters. We considered states to be partial adopters if any language clearly recognizable from the 2006 Decision Scheme (e.g. vehicular telemetry data consistent with a high risk or injury, time sensitive extremity injury) was present in any of their available field triage materials on the website (exceptions to this was when only a conjunction such as “and” or “or” was changed). We did not further stratify partial adopters. Next, we identified states that had some version (full or partial) of the 1999 field triage scheme on their website. Finally, we identified states with field triage schemes or methodology independent of the 1999 or 2006 schemes. Given the inherent language overlap in many of these latter two categories (1999 or other), the authors based their decisions regarding whether a scheme was consistent with 1999 on the language, flow, and organization of a given scheme.
For those states classified as either full or partial adopters, an analysis was performed using the U.S. Census Bureau’s “Annual Estimates of the Resident Population for the United States, July 1, 2009.”13We conducted this analysis to determine the percentage of the U.S. population living in an area with full or partial adoption of the 2006 Decision Scheme.
RESULTS
The authors located information regarding field triage on the publicly available websites for 41 states as of April 26, 2010. In nine states, the authors could not locate any information regarding field triage on their public websites.
Of the 41 states where authors located the information, seven (Arizona, Georgia, Indiana, Michigan, Tennessee, Utah and Virginia) were classified as “full adopters.” Nine were considered “partial adopters” (Arkansas, Delaware, Iowa, Maryland, Missouri, North Carolina, Pennsylvania, South Carolina and West Virginia). Authors found 17 states using a full version or modification of the 1999 Field Triage Decision Scheme8 (Alabama, Alaska, Colorado, Illinois, Kentucky, Maine, Massachusetts, Mississippi, Nebraska, New Jersey, New York, North Dakota, Ohio, Oklahoma, Oregon, South Dakota, Wisconsin). Reviewers judged that eight states (Florida, Hawaii, New Hampshire, New Mexico, Minnesota, Rhode Island, Vermont and Washington) were using a different protocol or scheme for field triage; the schemes were not clearly recognizable as versions of the 1999 or 2006 Field Triage Decision Schemes (Figure 4).

Based on the census data referenced above, states classified as full adopters represent 50,411,245 persons or 17% of the estimated 2009 U.S. population (303,039,262).13 States classified as partial adopters represent 45,016,379 persons or 15% of the estimated 2009 U.S. population (303,039,262 ).13
We conducted a further analysis of those states classified as full and partial adopters. The states of Arizona and Tennessee made no changes to the 2006 Field Triage Decision Scheme prior to placing it on their respective websites.14,15 Georgia adopted the 2006 Decision Scheme in its entirety, with only a minor addition to pediatric vital signs to Step one of the scheme, adding age specific criteria for the upper limit of respiratory rate in children under the age of six.16 Utah made minimal changes and added language to Steps one, three and four as well as the transition boxes.17 Although no protocol exists on its website, the EMS commission for Indiana has the legal authority from the state to “adopt rules concerning triage and transportation protocols for the transportation of trauma patients consistent with the field triage decision scheme of the ACS-COT”18 and passed a motion in September 2009 to “develop rule language that requires transport ambulance provider medical directors to issue protocols for the transportation of trauma patients consistent with the ACS-COT.”19 Similarly, in Michigan, the rules developed by the Michigan Department of Community Health governing the statewide trauma system state that “Protocols, which are established and adopted by local medical control, may be developed based on the standards incorporated by reference in these rules, Resources for Optimal Care Of The Injured Patient 2006.”20 Finally, the Office of EMS in Virginia in a 2009 review of triage processes within Virginia stated “Within this document [Resources for Optimal Care Of The Injured Patient 2006] is a triage scheme that has also been adopted by the CDC and NHTSA. The Office of Emergency Medical Services (OEMS) should use this document as it has the rest of the ACS/COT book and develop a statewide trauma triage scheme that will be incorporated into all EMS agencies patient care protocols in the applicable sections. This should in fact already be occurring.”21
In states classified as “partial adopters,” we found no consistency in the changes that were made. In some instances, the changes were minor. For instance, in South Carolina, the 2006 scheme was reproduced with a deletion from Step three (vehicular telemetry) and burns were not moved to Step four.22 In others, the scheme largely represents the 1999 scheme or a different triage algorithm, but contained language specific to the 2006 Field Triage Decision Scheme (e.g., vehicular telemetry data consistent with a high risk of injury, time sensitive extremity injury) within the algorithm. Some states, such as Delaware, incorporated many of the elements of the 2006 scheme, but presented them as an outline and eliminated the binary branch points contained in the original algorithm. The modified guideline is consistent with the flow and formatting of this state’s other prehospital protocols.23 In contrast, Pennsylvania maintained the overall structure of the algorithm, but combined the physiologic and anatomic elements into one category and the mechanism of injury and special consideration elements into a second category. The Pennsylvania guideline also added state specific destination and mode of transport criteria to the guideline.24 Similarly, the Arkansas triage scheme combined the physiologic and anatomic categories, and went into specific detail with respect to mode of transport, distance and time. However, unlike Pennsylvania, the Arkansas scheme is mostly derived from the 1999 document with a few elements from the 2006 Field Triage Decision Scheme.25
DISCUSSION
In its 2006 multi-volume report on the Future of Emergency Care in the United States, the Institute of Medicine called for the development of “model prehospital care protocols for the treatment, triage, and transport of patients.”26 Similarly, a multidisciplinary expert panel developed the 2006 Field Triage Decision Scheme in an effort to improve the field triage of injured patients across the U.S. It was endorsed by 17 national organizations, with concurrence from NHTSA. To the authors’ knowledge, the MMWR represents the first concerted effort to promulgate national guidelines for the field triage of injured patients.10
Following its original publication in the ACS-COT monograph Resources for the Optimal Care of the Injured Patient in 2006, the supporting rationale and evidence for the scheme was published in theMMWR in January 2009. 9–10 Following these publications, the CDC pursued an active plan for disseminating the 2006 Field Triage Decision Scheme. The CDC provided 250,000 field triage print materials including the MMWR, pocket card, posters and training guides to EMS medical directors, administrators and providers. The MMWR was reprinted in its entirety in JEMS: A Journal of Emergency Medical Services.27 Information regarding the Decision Scheme has been presented at international, national and regional conferences and has encouraged debate about the revisions contained in the 2006 version of the scheme.28 Additionally, the CDC established a website (www.cdc.gov/fieldtriage) in January 2009 that has had 47,193 page views and 4,953 downloads of the MMWR as of April 30, 2010.29
This paper represents the first attempt to analyze the use of the 2006 Field Triage Decision Scheme and provides insight into the scheme’s use, modifications and the population potentially covered by the field triage methodology.9 It also is a measure of the challenge of disseminating, translating, and implementing a national policy or guideline at the local level. This effort reveals that 32% of the 2009 U.S. population is living in a community that was identified in this study as having adopted (partially or fully) the 2006 Decision Scheme. Furthermore, the availability of such information to the general public could also be considered a ‘public notice’ of official administrative support for the 2006 Field Triage Decision Scheme within the governmental unit responsible for EMS.
For the prehospital environment, prior guideline development for this segment of healthcare providers has faced challenges. In a qualitative, exploratory study of EMS professionals at a national conference, Sasson et al.30 identified communication, uniform educational requirements and local EMS service coordination as potential operational barriers to the implementation of national guidelines for the termination of unsuccessful resuscitation efforts in the prehospital environment. Similarly, in a survey of 176 EMS agencies, Bingham et al.31 reported ten unique barriers to implementation of the 2005 American Heart Association guidelines for out-of-hospital cardiac arrest. The barriers fell into three categories including: instructional delays, technology delays regarding defibrillators, and decision-making delays at the state and local level.31 In addition, recent work by Weik32 among a national sample of pediatric emergency services providers, suggests that adoption and compliance can be enhanced. This may be done through the incorporation of local performance measures in the presence of state statutes, rules and regulations as well as the pivotal role of local emergency medicine ‘champions’ and existing job satisfaction by key EMS leaders.
There is a growing body of literature that examines the barriers and incentives for healthcare providers in the adoption, implementation and adherence to specific guidelines and clinical policies. In a 1999 article by Cabana et al.,33 32 years’ of published studies of barriers to guideline adoption were analyzed. This study found that while the reasons for guideline adherence may not be generalizable across specialties, there were common elements regarding the modification of physicians’ knowledge, attitudes, and behavior which could be addressed to reduce barriers to guideline adherence. Key issues such as lack of guideline awareness, familiarity, agreement, perceived self-efficacy and outcome expectancy in the context of institutional inertia and other external barriers were commonly reported. Furthermore, three Cochrane systematic reviews in the past two years, not only have confirmed these earlier findings, but also offer evidence to suggest that adoption and compliance may be improved by tailoring interventions to a given locality rather than at a national level.34–36 However, the present study was unable to examine specific barriers to adoption of the scheme using the available methodology. Further evaluation of barriers is needed, and would certainly affect the development and execution of policies or programs designed to increase adaptation and strengthen implementation of not only these, but also additional guidelines targeting the prehospital environment.
LIMITATIONS
This study has several important limitations. Our methodology consisted only of internet searches of publicly available information. Location of relevant material not only depended upon the authors’ ability to navigate to and locate the necessary information, but also on website design, maintenance, and content updates. Some states may have endorsed, adopted, or used the 2006 Field Triage Decision Scheme; however, these activities may not be adequately or appropriately reflected on their public websites. Thus, some states classified as “information not available” or using a different scheme, may in fact be using the 2006 Field Triage Decision Scheme, but they did not have that information readily available on their website. The states that actually use other guidelines may not be aware of the revisions or they simply may not have had time to update their guidelines on their respective websites. The authors did not conduct a formal survey of state health departments or EMS agencies, which may have provided more information regarding the current status of the adoption and use of the 2006 Decision Scheme. However, we thought that if information was not publicly available, then the dissemination and adoption of the guideline may not have occurred statewide. We acknowledge that placement of the 2006 Field Triage Decision Scheme on a website does not guarantee that the scheme is being used throughout a state. States vary in regulatory nature regarding the provision of EMS. Thus, a state may not be able to mandate use of the 2006 scheme within their local communities, and placement of the Decision Scheme on the website may not accurately reflect activities at the local level. Finally, we were not able to compare the speed and spread of adoption to prior revisions. In the past, the guideline has simply been part of the ACS-COT book Resources for the Optimal Care of the Injured Patient but there have not been the same extensive dissemination efforts that were used for the 2006 guideline.4,6–9 However, given that at least eight states in this study used their own version of a field triage guideline, this suggests that there are states that are either not aware of the national guideline, or may not consider that the national guideline meets their needs.
CONCLUSION
Accurate field triage is critical. Getting the right person, to the right place, at the right time can have a profound impact on patient morbidity and mortality as well as overall system efficiency, effectiveness, and safety.3 The 2006 Field Triage Decision Scheme incorporates a rigorous review of the available science on field triage and represents the multidisciplinary expertise of individuals across the spectrum of public health and acute injury care. Many states have adopted the 2006 Decision Scheme either fully or partially. However, further investigation is needed to determine the reasons why some states may choose not to adopt the guidelines and whether such a decision represents a need for more enhanced guideline dissemination or incorporation of perceived local needs and considerations.
Footnotes
Supervising Section Editor: Monica H Swahn, PhD, MPH
Submission history: Submitted: January 20, 2011; Revision received March 3, 2011; Accepted March 3, 2011.
Reprints available through open access at http://escholarship.org/uc/uciem_westjem.
Address for Correspondence: Marlena Wald, MLS, MPH
Division of Injury Response, National Center for Injury Prevention and Control, CDC, 4770 Buford Highway, MS F-62, Atlanta, GA 30341-3717
Email: mmwald@cdc.gov
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. US Dept of Health and Human Services. Centers for Disease Control and Prevention. WISQARS: web-based injury statistics query and reporting system: leading causes of death reports, 2007.Atlanta, GA: CDC; 2010. Available at: http://www.cdc.gov/injury/wisqars/index.html Accessed: June 3, 2010.
2. US Dept of Health and Human Services. Centers for Disease Control and Prevention. National Center for Health Statistics. National Hospital Ambulatory Care Survey: 2007. (NHAMCS) Hyattsville, MD: National Center for Health Statistics; 2007.
3. MacKenzie EJ, Rivara FP, Jurkovich GJ, et al. A national evaluation of the effect of trauma center care on mortality. N Engl J Med. 2006;354:366–78. [PubMed]
4. American College of Surgeons. Hospital and prehospital resources for the optimal care of the injured patient: appendices A through J. Chicago, IL: American College of Surgeons; 1986.
5. Mackersie RC. History of trauma field triage development and the American College of Surgeons criteria. Prehosp Emerg Care. 2006;10:287–94. [PubMed]
6. American College of Surgeons. Resources for the optimal care of the injured patient: 1990.Chicago, IL: American College of Surgeons; 1990.
7. American College of Surgeons. Resources for the optimal care of the injured patient: 1993.Chicago, IL: American College of Surgeons; 1993.
8. American College of Surgeons. Resources for the optimal care of the injured patient: 1999.Chicago, IL: American College of Surgeons; 1999.
9. American College of Surgeons. Resources for the optimal care of the injured patient: 2006.Chicago, IL: American College of Surgeons; 2006.
10. US Dept of Health and Human Services. Centers for Disease Control and Prevention. Guidelines for field triage of injured patients: Recommendations of the National Expert Panel on Field Triage.MMWR. 2009;58(RR-1):1–35.
11. American Association of Law Libraries. Government Relations Office and Washington Affairs Office. State-by-State Report on Permanent Public Access to Electronic Government Information.2003. Available at: http://www.aallnet.org/aallwash/PPAreport.asp Accessed: Feb 10, 2010.
12. Neilsen Company. Top U.S. online search providers home & work:April, 2010. Neilsen Insights.Available at: http://en-us.nielsen.com/rankings/insights/rankings/internet. Last accessed: June 3, 2010.
13. US Dept of Commerce. Bureau of the Census. Annual estimates of the resident population for the United States, regions, states, and Puerto Rico: April 1, 2000 to July 1, 2009. Available at:http://www.census.gov/popest/states/NST-ann-est.html Last accessed: June 3, 2010.
14. Tennessee Department of Health, Trauma. Available at:http://health.state.tn.us/ems/PDF/g4183036.pdf. Last accessed April 26, 2010.
15. Arizona Department of Health Services, Division of Public Health Services, Bureau of Emergency Medical Services and Trauma System. Available at: http://www.azdhs.gov/bems/trauma-pdf/GuidelinesFieldTriage.pdf. Last accessed April 26, 2010.
16. Georgia Department of Human Resources, Division of Public Health Office of Emergency Medical Services/Trauma. Emergency Pre-Hospital Protocols. Available at:http://www.vdh.virginia.gov/OEMS/Files_page/trauma/TraumaTriageReport01-09.pdf. Last accessed April 26, 2010.
17. Utah Department of Health, Bureau of Emergency Medical Services. Resources and Guidelines for the Triage and Transfer of Trauma Patients. Available at:http://health.utah.gov/ems/trauma/triage_transfer_guidelines.pdf. Last accessed April 26, 2010.
18. Indiana General Assembly; Indiana Emergency Medical Services Commission. Available at:http://www.in.gov/legislative/ic/code/title16/ar31/ch2.html. Last accessed April 26, 2010.
19. Indiana Department of Homeland Security EMS. Available at:http://www.in.gov/dhs/files/trauma_field_triage_draft3.pdf. Last accessed April 26, 2010.
20. Michigan Department of Community Health, Statewide Trauma System. Available at:http://www.michigan.gov/documents/Draft_Administrative_Trauma_Rules_5_156468_7.0.pdf. Last accessed April 26, 2010.
21. Virginia Department of Health; Office of Emergency Medical Services. Available at:http://www.vdh.virginia.gov/OEMS/Files_page/trauma/TraumaTriageReport01-09.pdf. Last accessed April 26, 2010.
22. South Carolina Department of Health and Environmental Control; South Carolina Emergency Medical Services. Available at: http://www.scdhec.gov/health/ems/TraumaLetterScheme.pdf. Last accessed April 26, 2010.
23. Delaware Health and Social Services; Division of Public Health. Office of Emergency Medical Services. Statewide Standard Treatment Protocols. Available at:http://www.dhss.delaware.gov/dph/ems/ems.html. Last accessed April 26, 2010.
24. Pennsylvania Department of Health; Bureau of Emergency Medical Services; Pennsylvania Statewide Basic Life Support Protocols. Available at:http://www.portal.state.pa.us/portal/server.pt/community/emergency_medical_services/14138/ems_statewide_protocols/625966. Last accessed April 26, 2010.
25. Arkansas Department of Health; Emergency Medical Services and Trauma Systems; Rules and Regulations for Trauma Systems. Available at:http://www.healthy.arkansas.gov/programsServices/hsLicensingRegulation/EmsandTraumaSystems/Pages/default.aspx. Last accessed April 26, 2010.
26. Institute of Medicine. Committee on the Future of Emergency Care in the United States Health System Future of Emergency Care. Vol. 3. Washington, D.C: National Academies Press; 2006.
27. Sasser SM, Hunt RC, Sullivent EE, et al. Guidelines for field triage of injured patients. Recommendations of the National Expert Panel on field triage. JEMS. 2009 Jul;34(7):1–35. (suppl) (quiz): 36–9.
28. Champion HR, Lombardo LV, Shair EK. The importance of vehicle rollover as a field triage criterion. J Trauma. 2009 Aug;67(2):350–7. [PubMed]
29. US Dept of Health and Human Services; Centers for Disease Control and Prevention; National Center for Injury Prevention and Control. Field Triage Decision Scheme. Available at:http://www.cdc.gov/fieldtriage/index.html Last accessed: April 9, 2010.
30. Sasson C, Forman J, Krass D, et al. A qualitative study to understand barriers to implementation of national guidelines for prehospital termination of unsuccessful resuscitation efforts. Prehosp Emerg Care. 2010 Apr 6;14(2):250–8. [PubMed]
31. Bingham BL, Aufderheide TP, Donn S, et al. Barriers to guideline implementation: A qualitative survey of emergency medical services [abstract] Circulation. 2008 Oct 28;118(18):822. (suppl) Abstract 4034.
32. Weik TS. Measuring the barriers and facilitators in the implementation of performance measures in emergency medical services for children [dissertation] Washington, DC: The George Washington University; 2009.
33. Cabana MD, Rand CS, Powe NR, et al. Why don’t physicians follow clinical practice guidelines?: A framework for improvement. JAMA. 1999;282(15):1458–65. [PubMed]
34. Shaw B, Cheater F, Baker R, et al. Tailored interventions to overcome identified barriers to change: Effects on professional practice and health care outcomes. Cochrane Database Syst Rev.2005 Jul 20;(3):CD005470. [PubMed]
35. O’Brien MA, Rogers S, Jamtvedt G, et al. Educational outreach visits: Effects on professional practice and health care outcomes. Cochrane Database Syst Rev. 2007 Oct 17;(4):CD000409.[PubMed]
36. Forsetlund L, Bjorndal A, Rashidian A, et al. Continuing education meetings and workshops: Effects on professional practice and health care outcomes. Cochrane Database Syst Rev. 2009 Apr 15;(2):CD003030. [PubMed]