
{kind=link}
| Author | Affiliation |
|---|---|
| Jonathan Rowland, MD | Wayne State University School of Medicine, Department of Emergency Medicine, Detroit, Michigan |
| Dean Fouchia, MD | Wayne State University School of Medicine, Department of Emergency Medicine, Detroit, Michigan |
| Mark Favot, MD | Wayne State University School of Medicine, Department of Emergency Medicine, Detroit, Michigan |
ABSTRACT
Case Presentation
An eight-week-old infant presented to the emergency department in cardiac arrest. Return of spontaneous circulation was obtained and the patient subsequently began seizing. Point-of-care ultrasound of the anterior fontanelle revealed an extra-axial fluid collection consistent with subdural hematoma (SDH).
Discussion
Abusive head trauma is still frequently missed on initial presentation. In addition to validated screening clinical prediction rules, point-of-care cranial ultrasound can be used as a noninvasive adjunct for detection of SDH related to abusive head trauma in infants with an open fontanelle.
CASE PRESENTATION
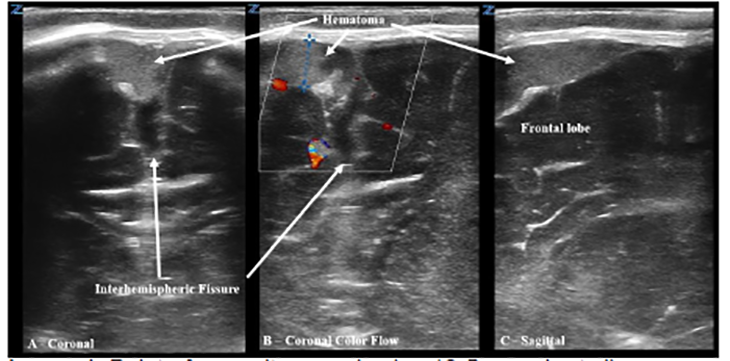
An eight-week-old male with a history of laryngomalacia and prematurity born at 36 weeks presented to the emergency department (ED) in cardiac arrest after being found unresponsive at home. Cardiopulmonary resuscitation was initiated on arrival to the ED, intraosseous access was established, and the patient was intubated with subsequent return of spontaneous circulation. Ten minutes later, he had a generalized tonic-clonic seizure, and the anterior fontanelle was noted to be tense. Point-of-care ultrasound (POCUS) of the anterior fontanelle revealed an echogenic extra-axial fluid collection suspected to represent subdural hematoma (SDH) (Image 1).
The patient was successfully stabilized, then transferred to a tertiary center where a computed tomography (CT) of the brain confirmed the presence of an SDH, intraparenchymal hemorrhages of the hypothalamus and brainstem, and an anterior neck hematoma concerning for non-accidental trauma (Image 2).

DISCUSSION
Diagnosis: Acute Subdural Hematoma in Setting of Non-accidental Trauma
Abusive head trauma (AHT) is the leading cause of fatal head injuries in children under two years, with SDH being the most frequently identified lesion (up to 90%) located most commonly in the parafalcine space along the superior sagittal sinus.1 The rate of missed AHT remains largely unchanged for the last 20 years at roughly 30%.2 Best practice recommendation is to avoid applying PECARN head CT rule3 to any suspected victims of AHT, and to instead use the validated “TEN-4 FACESp”4 clinical prediction tool to maximize sensitivity in detection of sentinel injuries predictive of abuse.2 Emergency physicians have been demonstrated as capable of identifying intracerebral hemorrhage using POCUS.5,6 POCUS should be considered when evaluating infants with suspected AHT or new-onset seizures and is easily performed with brief examination of the parafalcine space through the anterior fontanelle window using a high-frequency linear probe.
CPC-EM Capsule
What do we already know about this clinical entity?
Subdural hematoma is the most commonly identified lesion in fatal cases of abusive head trauma (AHT). The rate of missed AHT remains largely unchanged (~30%) for the last twenty years.
What is the major impact of the image(s)?
Point-of-care ultrasound (POCUS) can be utilized in infants with open fontanelles and should be considered in evaluation of suspected AHT and/or undifferentiated new-onset seizures.
How might this improve emergency medicine practice?
POCUS can be utilized as a noninvasive adjunct, in addition to validated clinical prediction tools, to improve our detection of AHT.
Footnotes
Section Editor: Rick McPheeters, DO
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
The authors attest that their institution requires neither Institutional Review Board approval, nor patient consent for publication of this image in emergency medicine. Documentation on file.
Address for Correspondence: Jonathan Rowland, MD, Wayne State University School of Medicine, Department of Emergency Medicine, 6071 W. Outer Dr., Lourdes 447-D, Detroit, MI 48235. Email: jrowland@dmc.org. 4:485 – 486
Submission history: Revision received May 14, 2020; Submitted June 10, 2020; Accepted June 17, 2020
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Choudhary A, Servaes S, Slovis T, et al. Consensus Statement on Abusive Head Trauma in Infants and Young Children. Pediatr Radiol. 2018;48(8):1048-65.
2. Berger RP, Lindberg DM. Early recognition of physical abuse: bridging the gap between knowledge and practice. J Pediatr. 2019;204:16-23.
3. Kuppermann N, Holmes J, Dayan P, et al. Identification of children at very low risk of clinically-important brain injuries after head trauma: a prospective cohort study. Lancet. 2009;374(9696):1160-70.
4. Pierce M, Kaczor K, Lorenz D, et al. Bruising Clinical Decision Rule (BCDR) discriminates physical child abuse from accidental trauma in young children.
5. McCormick T, Chilstrom M, Childs J, et al. Point-of-care ultrasound for the detection of traumatic intracranial hemorrhage in infants. Pediatr Emer Care. 2017;33(1):18-20.
6. Lee S, Bellamkonda Athmaram VR, Anderson JL. Infant with limpness; subdural hemorrhage from suspected abusive head trauma. Ann Emerg Med. 2013;61(1):18-36.
SUPPLEMENTARY MATERIAL
Coronal sweep of the anterior fontanelle with a high-frequency linear 10-5 MHz probe utilizing color doppler to evaluate flow around the subdural hematoma within the interhemispheric fissure/parafalcine space.
Coronal sweep of the anterior fontanelle at the interhemispheric fissure/parafalcine space with a high-frequency linear 10-5 MHz probe with B-mode imaging, demonstrating a subdural hematoma to the right of midline with associated widening of the interhemispheric fissure.
Sagittal sweep of the anterior fontanelle at the frontal lobe with a high-frequency linear 10-5 MHz probe with B-mode imaging, demonstrating an echogenic subdural hematoma.