
{kind=link}
| Author | Affiliation |
|---|---|
| Jessica Lynn Williams, MD | Saint Joseph’s University Medical Center, Emergency Department, Paterson, New Jersey |
| Steven M. Hochman, MD | Saint Joseph’s University Medical Center, Emergency Department, Paterson, New Jersey |
ABSTRACT
Case Presentation
In this case, we demonstrate how a small radiolucency in the proximal humerus can progress to an even larger problem within a few months in a patient without follow-up. Our patient’s ultimate diagnosis was renal cell carcinoma with metastasis to the right proximal humerus, completely obliterating the affected bone.
Discussion
In many underserved communities, patients have limited access to medical care, particularly specialty care. These patients often present to the emergency department and are unable to acquire appropriate follow-up. This situation illustrates the social issues that our patients face every day affecting their access to healthcare and ultimately necessary medical treatment.
CASE PRESENTATION
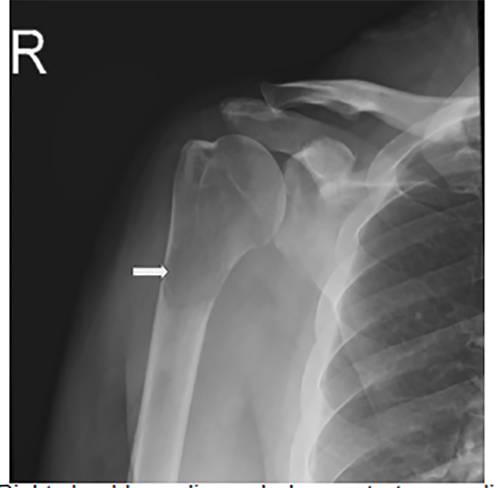
A 56-year-old male with a history of alcoholic liver cirrhosis presented to the emergency department (ED) for worsening atraumatic right proximal arm pain. His examination was remarkable for limited active and passive range of motion of the right shoulder. He had presented to an affiliated ED three months prior for similar complaints. At that time, radiographs demonstrated a radiolucency in the right proximal humerus (Image 1). Computed tomography on the same date demonstrated a metastatic or a primary bone lesion.
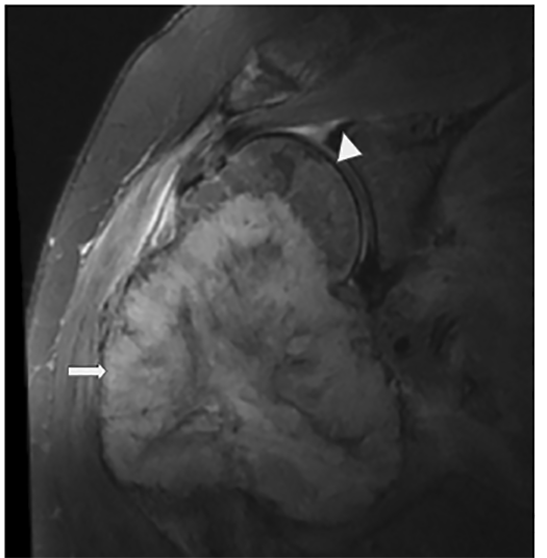
The patient was discharged and instructed to follow up as an outpatient, but was unable to do so. The radiograph of the right humerus on the current visit demonstrated a large, soft tissue lytic mass (Image 2). The patient was admitted to the hospital and diagnosed with renal cell carcinoma (RCC) of the right kidney with metastasis to the humerus. Magnetic resonance imaging of the right humerus four days after admission can be seen in Image 3. The patient underwent right radical resection of the right proximal humerus mass, reverse total shoulder arthroplasty and rotator cuff repair at another institution. Pathology reports confirmed the humeral mass was metastatic RCC. The patient was started on infusion therapy.

DISCUSSION
RCC is responsible for 3% of all cancers.1 Bone metastasis is most commonly from breast, prostate, and lungs.2 However, 25–30% of RCC tumors metastasize to bone.1 Emergency physicians should have a low threshold for obtaining radiographs in patients with atraumatic pain to rule out pathologic lesions. With a five-year RCC survival rate of less than 50%, early detection and initiation of treatment are essential, as earlier stages of cancer have better survival rates and treatment options. If patients lack follow-up or insurance, emergency providers must be diligent to provide patient education and assist in arranging follow-up for a better chance of survival.
CPC-EM Capsule
What do we already know about this clinical entity?
Once cancer becomes stages 3 or 4 with metastasis, there are fewer treatment options and lower survival rates.
What is the major impact of the image(s)?
Subtle nonspecific findings on plain films can be early indications of pathology that can progress rapidly, reinforcing the importance of early diagnosis and treatment.
How might this improve emergency medicine practice?
Imaging should be obtained for atraumatic pain in patients with limited access to follow-up care who present with insidious onset or whose pain occurs at night or is not relieved by conservative treatment.
Footnotes
Section Editor: Rick A. McPheeters, DO
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
The authors attest that their institution requires neither Institutional Review Board approval, nor patient consent for publication of this image in emergency medicine. Documentation on file.
Address for Correspondence: Jessica L. Williams, MD, Saint Joseph’s University Medical Center, Department of Emergency Medicine, 703 Main Street, Paterson, NJ 07503. Email: jlwilliams4@geisinger.edu. 4:487 – 488
Submission history: Revision received May 23, 2020; Submitted June 3, 2020; Accepted June 18, 2020
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Umer M, Mohib Y, Atif M, et al. Skeletal metastasis in renal cell carcinoma: A review. Ann Med Surg (Lond). 2018;27:9-16.
2. Nielsen OS, Munro AJ, Tannock IF. Bone metastases: pathophysiology and management policy. J Clin Oncol. 1991;9(3):509-24.