
{kind=link}
| Author | Affiliation |
|---|---|
| Megan Gillespie, DO | Jefferson Health – Northeast, Department of Emergency Medicine, Philadelphia, Pennsylvania |
| Patrick Flannery, DO | Jefferson Health – Northeast, Department of Emergency Medicine, Philadelphia, Pennsylvania |
| Jessica A. Schumann, DO | Jefferson Health – Northeast, Department of Emergency Medicine, Philadelphia, Pennsylvania |
| Nathan Dincher, DO | Jefferson Health – Northeast, Department of Emergency Medicine, Philadelphia, Pennsylvania; Jefferson Health – Northeast, Department of Critical Care, Philadelphia, Pennsylvania |
| Rebecca Mills, MD | Jefferson Health – Northeast, Department of Emergency Medicine, Philadelphia, Pennsylvania |
| Argun Can, MD | Jefferson Health – Northeast, Department of Critical Care, Philadelphia, Pennsylvania |
ABSTRACT
Introduction
Coronavirus disease 2019 (COVID-19) is caused by severe acute respiratory syndrome coronavirus 2.1 COVID-19 first occurred in Wuhan, China, in December 2019, and by March 2020 COVID-19 was declared a global pandemic.1
Case Presentation
We describe a case of a 52-year-old female with past medical history of asthma, type 2 diabetes, and previous tobacco use who presented to the emergency department with dyspnea and was found to be positive for COVID-19. We discuss the computed tomographic finding of “crazy-paving” pattern in the patient’s lungs and the significance of this finding in COVID-19 patients.
Discussion
Emergency providers need to be aware of the different imaging characteristics of various stages of COVID-19 to appropriately treat, isolate, and determine disposition of COVID-19 infected patients. Ground-glass opacities are the earliest and most common imaging finding for COVID-19.2–4 Crazy-paving pattern is defined as thickened interlobular septa and intralobular lines superimposed on diffuse ground-glass opacities and should be recognized by emergency providers as a radiographic finding of progressive COVID-19.2–4
CASE PRESENTATION
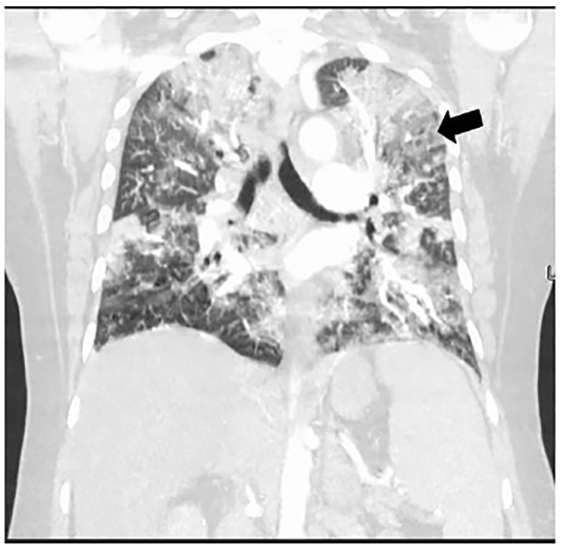
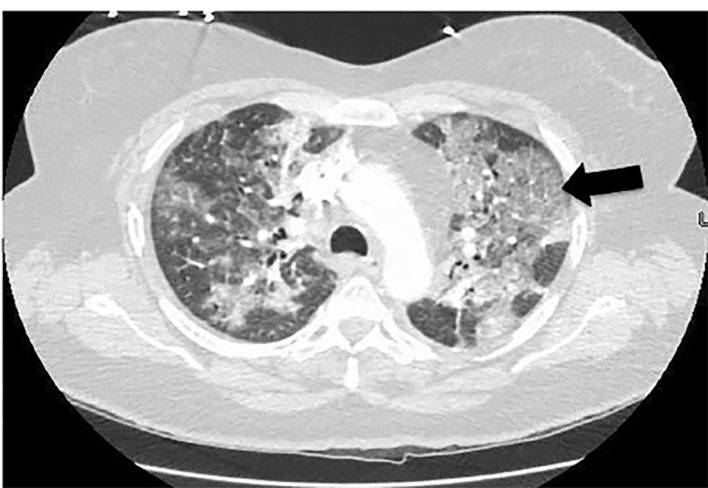
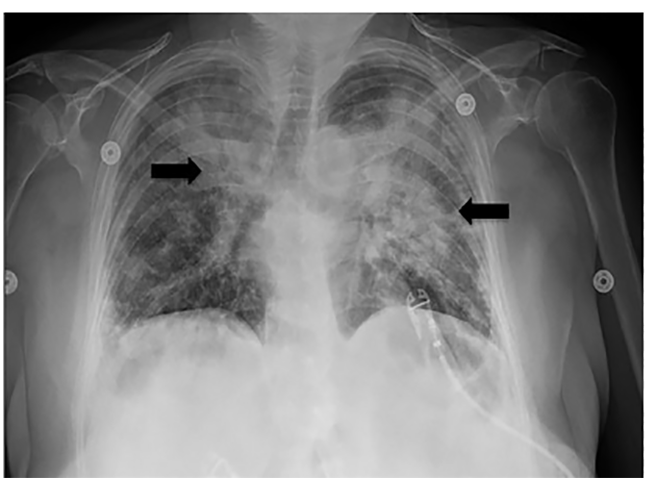
A 52-year-old female with past medical history of asthma, type 2 diabetes, and previous tobacco use presented to the emergency department with dyspnea. The patient denied fever/chills, congestion, or gastrointestinal symptoms. She denied recent travel or exposure to known sick contacts. She presented afebrile, tachycardic, tachypneic, hypoxic with pulse oximetry measuring 79% on room air, and had mild conversational dyspnea with diminished auscultated breath sounds bilaterally. The patient had imaging findings as below (Images 1, 2, and 3) and laboratory abnormalities of elevated D-dimer, fibrinogen, lactate dehydrogenase, ferritin, C-reactive protein, lactic acid, glucose, aspartate aminotransferase, and alanine aminotransferase, in conjunction with a positive severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) reverse transcriptase polymerase chain reaction assay.
The patient was started on mid-flow supplemental nasal cannula oxygen at 15 liters per minute, enoxaparin, azithromycin, and ceftriaxone, and was admitted to the hospital.
DISCUSSION
Coronavirus disease 2019 (COVID-19) is caused by SARS-CoV-2.1 The COVID-19 outbreak first occurred in Wuhan, China, in December 2019, and by March 2020, COVID-19 was declared a global pandemic.1 Emergency physicians are on the front line to diagnose and treat this global health emergency. These images are intended to present the “crazy-paving” pattern, which is a computed tomographic (CT) finding of progressive COVID-19.
CPC-EM Capsule
What do we already know about this clinical entity?
Ground-glass opacities are the most common and frequently noted radiographic abnormality of corona virus disease 2019 (COVID-19).
What is the major impact of the image(s)?
Crazy-paving pattern – thickened interlobular septa and intralobular lines superimposed on diffuse ground-glass attenuation – is an imaging finding suggestive of progressive COVID-19.
How might this improve emergency medicine practice?
Awareness of imaging findings of COVID-19 will help providers appropriately treat, isolate, and determine the disposition of infected patients promptly.
Ground-glass opacities, defined as hazy opacities compared to healthy lung, are the earliest and most commonly noted finding on CT for COVID-19.2-4 As COVID-19 progresses, a pattern known as “crazy-paving” can be noted on CT.3-4 Crazy-paving is defined by the Fleischner Society as thickened interlobular septa and intralobular lines superimposed on diffuse ground-glass attenuation, and is named for its resemblance to stone pavement streets.2-5 Crazy-paving pattern is classically noted as a finding of pulmonary alveolar proteinosis, a rare lung disease, but this pattern is also caused by Pneumocystis jiroveci pneumonia, sarcoidosis, bronchioloalveolar carcinoma, amiodarone-induced nonspecific interstitial pneumonia, lipoid pneumonia, organizing pneumonia, acute respiratory distress syndrome, pulmonary hemorrhage syndromes, and, now, COVID-19.3-5
Footnotes
Section Editor: Rick A. McPheeters, DO
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
The authors attest that their institution requires neither Institutional Review Board approval, nor patient consent for publication of this image in emergency medicine. Documentation on file.
Address for Correspondence: Megan Gillespie, DO, Jefferson Health – Northeast, Department of Emergency Medicine, Graduate Medical Education Office, ℅ Mary Allegrini, 10800 Knights Road, Philadelphia, PA 19114. Email: megan.gillespie@jefferson.edu. 4:461 – 463
Submission history: Revision received May 1, 2020; Submitted May 11, 2020; Accepted May 11, 2020
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Coronavirus disease 2019 (COVID-19) pandemic. 2020. Available at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019. Accessed May 1, 2020.
2. Hansell DM, Bankier AA, MacMahon H, et al. Fleischner Society: glossary of terms for thoracic imaging. Radiology. 2008;246(3):697-722.
3. Ye Z, Zhang Y, Wang Y, et al. [Ahead of Print]. Chest CT manifestations of new coronavirus disease 2019 (COVID-19): a pictorial review. Eur Radiol. 2020.
4. Salehi S, Abedi A, Balakrishnan S, et al. [Ahead of Print]. Coronavirus disease 2019 (COVID-19): a systematic review of imaging findings in 919 patients. AJR Am J Roentgenol. Accessed March 14, 2020.
5. Rossi SE, Erasmus JJ, Volpacchio M, et al. “Crazy-paving” pattern at thin-section CT of the lungs: radiologic-pathologic overview. RadioGraphics. 2003;23(6):1509-19.