
{kind=link}
| Author | Affiliation |
| John Ashurst, DO | Lehigh Valley Health Network, Allentown, Pennsylvania |
| Kevin Weaver, DO | Lehigh Valley Health Network, Allentown, Pennsylvania |
A 77 year-old woman presented with a one day history of central chest pressure that radiated to the neck and right upper extremity. She had a history of hypertension and chronic obstruction pulmonary disease. Her blood pressure was 86/47 with a heart rate of 87 beats per minute. A grade 2/6 systolic ejection murmur was auscultated over the left sternal border. An electrocardiogram showed ST elevation in lead III with ST depression I, AVL, V4-V6 and a chest radiograph was obtained which showed an “egg shell sign” as compared to previous radiograph (Figures 1 and 2). The patient was diagnosed with a type A aortic dissection and taken to the operating room for emergent repair but died during the procedure.
DISCUSSION
Aortic dissection was first described more than 200 years ago by Morgagni and since then has become the most common aortic emergency requiring surgical intervention.1,2 Aortic dissections are currently classified by their location with the Stanford Type A dissection involving the ascending aorta, and the Type B dissection occurring distal to the left subclavian artery.2
A meta-analysis showed that acute onset of pain had a sensitivity of 84% and that severe pain had a sensitivity of 90% for aortic dissection.3 A new diastolic murmur does little to change the pretest probability but pulse deficits or a blood pressure differential has a high pre-test probability of aortic dissection.3 Chest radiography is abnormal in 90% of patients with an acute aortic dissection.3 In Figure 2, the patient had both a widened mediastinum and an “egg shell” sign indicative of an aortic dissection. The “egg shell” sign is reported in only 14% of patients with aortic dissection and is described as displacement of the soft tissue greater than 6mm from an aortic calcification.2,4

Figure 1. Previous radiograph with no acute disease process.
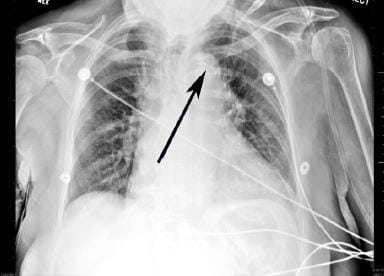
Figure 2. Egg shell sign (arrow), defined as a distance greater than 6mm from the aortic calcification to the lateral soft tissue margin of the aorta, with a widened mediastinum indicating aortic dissection.
Footnotes
Supervising Section Editor: Sean O. Henderson, MD
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: John Ashurst, DO, Lehigh Valley Health Network, 2545 Schoenersville Rd, Bethlehem, PA 18017-7300. Email: ashurst.john.32.research@gmail.com.
Submission history: Submitted May 17, 2014; Revision received June 9, 2014; Accepted September 1, 2014
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
- Leonard JC. Thomas Bevill Peacock and the early history of dissecting aneurysm. BMJ.1979;2:260-262. [PubMed]
- Hagan PG, Nienaber CA, Isselbacher EM, et al. The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease. JAMA. 2000;283(7):897-903. [PubMed]
- Klompas M. Does this patient have an acute thoracic aortic dissection. JAMA. 2002;287(17):2262-2272. [PubMed]
- Umeki S. A new roentgenographic sign: the split eggshell sign for aortic arch aneurysms. Am J Med. 1989;86(3):362–363. [PubMed]