
{kind=link}
| Author | Affiliation |
|---|---|
| Siri Shastry, MD | University of California, Irvine, Department of Emergency Medicine, Irvine, California |
| Kristi L. Koenig, MD | University of California, Irvine, Department of Emergency Medicine, Irvine, California |
Starting in 2015, microcephaly associated with Zika virus emerged as a public health emergency of international concern. Initial cases in the United States were travel-associated; however, there are increasing reports of local transmission in pockets of the country, and therefore public concerns may escalate.1 Emergency physicians commonly perform point-of-care ultrasound (POCUS) on pregnant patients, a population of special concern. This paper describes ultrasound findings typical of Zika-related congenital malformations that may be incidental findings or detected when examining exposed or concerned patients during routine POCUS testing. These concerns should alert emergency physicians to assess for Zika-virus risk factors and provide urgent referral for confirmatory studies and counseling if indicated.
Fetal microcephaly and other congenital malformations are devastating consequences of Zika virus infection.2 As the number of cases of Zika virus within the United States increases from either travel or local transmission, emergency physicians (EP) may encounter an increased population of pregnant females with a history of exposure to the virus either via mosquito bites, sexual transmission or possibly even transfusion-related. Pregnant patients may present to the emergency department (ED) either with perceived or real exposures to Zika virus infection. Point-of-care ultrasound (POCUS) performed either on these concerned patients or on any pregnant patient for routine indications may reveal incidental findings consistent with Zika-associated congenital abnormalities. As up to 80% of patients infected with Zika virus are asymptomatic, pregnant patients may be unaware they have contracted the virus.3 Further, any pregnant female with a possible exposure to Zika virus may present with questions regarding the nature of possible complications as well as regarding follow-up care. Therefore, for purposes of counseling and referral, it is important that EPs be knowledgeable about ultrasound findings associated with congenital Zika virus infection as well as indications for urgent referral for confirmatory testing.
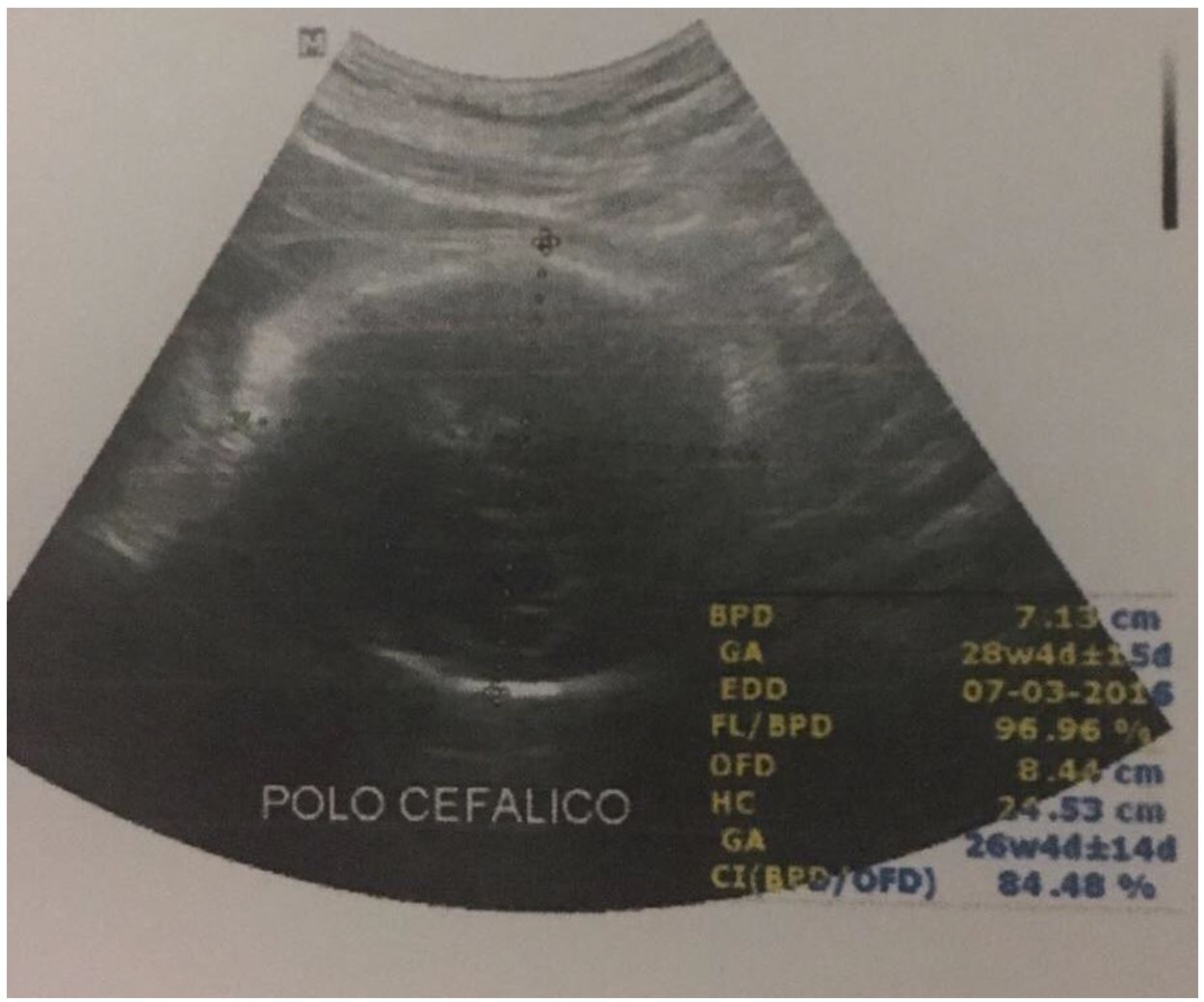
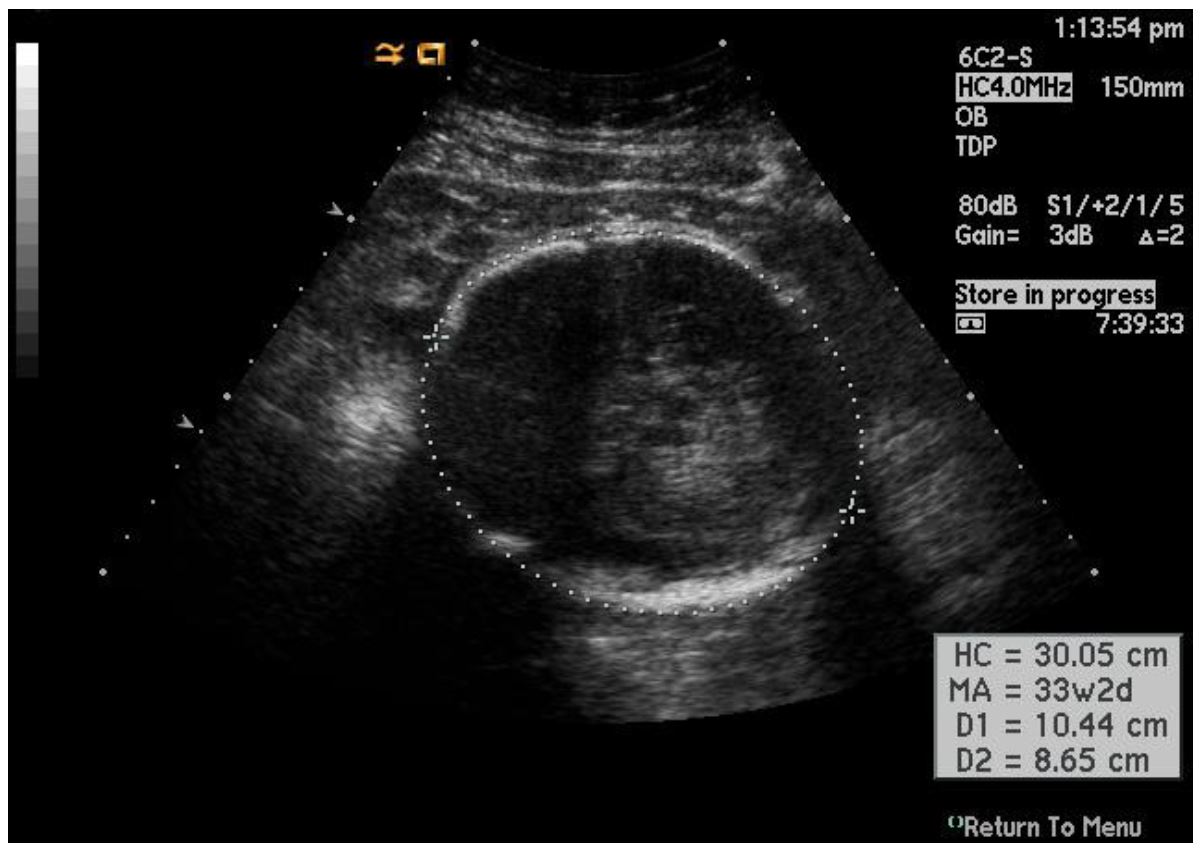
Ultrasound findings in fetuses with congenital Zika virus infection include microcephaly, intracranial calcifications, ventriculomegaly and arthrogyposis, as well as abnormalities of the corpus callosum, cerebrum/cerebellum and eyes (Images 1 and 2).4,5 Fetal microcephaly is defined as a head circumference measurement either less than two standard deviations below the average head circumference or below the third percentile for sex and gestational age.6 Microcephaly can be detectable as early as 18–20 weeks gestational age. Diagnostic utility of US increases as gestational age increases. Even in the absence of microcephaly, the presence of intracranial calcifications prior to 22 weeks gestational age may predict its future development.4 While presence of suspicious findings should prompt urgent referral, regardless of bedside US appearance, all women concerned about Zika virus infection should be referred to an obstetrician for further testing and formal US evaluation. Timing of exposure/presentation as well as serologic testing results will determine whether routine obstetric US or serial US are indicated.5
While the detection of specific point-of-care fetal ultrasound findings associated with Zika virus disease is beyond the scope of knowledge expected for EPs, any unusual appearance should prompt an assessment of the patient’s risk factors for the infection. This is particularly critical as the vast majority of patients will be asymptomatic. Through knowledge of US findings indicative of Zika-virus related congenital malformations, EPs will be empowered to facilitate timely referrals for concerned or possibly exposed pregnant patients who may otherwise only present to the ED for routine POCUS testing.
Footnotes
Section Editor: Rick A. McPheeters, DO
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
Address for Correspondence: Siri Shastry, MD, University of California Irvine Medical Center, 333 The City Blvd. West, Suite 640, Orange, CA 92868. Email: spshastr@uci.edu. 1:71 – 72
Submission history: Revision received October 20, 2016; Accepted November 28, 2016
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Case Counts in the US. Available at: http://www.cdc.gov/zika/geo/united-states.html. Accessed Sept 6, 2016.
2. Rasmussen SA, Jamieson DJ, Honein MA, et al. Zika virus and birth defects – reviewing the evidence for causality. N Engl J Med. 2016;374(20):1981-7.
3. Shastry S, Koenig KL, Hirshon JM. Zika virus: critical information for emergency providers. Emerg Med Clin North Am. 2016;34(3):E25-37.
4. Prenatal Diagnosis of Microcephaly. Available at: http://www.cdc.gov/zika/hc-providers/pregnant-women/prenatal-diagnosis-microcephaly.html. Accessed Sept 6, 2016.
5. Practice Advisory on Zika Virus. Available at: http://www.cdc.gov/zika/hc-providers/pregnant-women/prenatal-diagnosis-microcephaly.html. Accessed Sept 6, 2016.
6. Facts about Microcephaly. Available at: http://www.cdc.gov/birthdefects/microcephaly.html. Accessed Nov 20, 2016.
7. Villar J, Cheikh IL, Victoria CG, et al. International standards for newborn weight, length, and head circumference by gestational age and sex: the Newborn Cross-Sectional Study of the INTERGROWTH-21 Project. Lancet. 2014;384(9946):857-68.