
{kind=link}
| Author | Affiliation |
|---|---|
| Imran Asad, MD | University of Toronto, Hospital for Sick Children, Division of Pediatric Emergency Medicine, Department of Pediatrics, Toronto, Canada |
| Michelle Sin Lee, MDCM | University of Toronto, Hospital for Sick Children, Division of Pediatric Emergency Medicine, Department of Pediatrics, Toronto, Canada |
CASE PRESENTATION
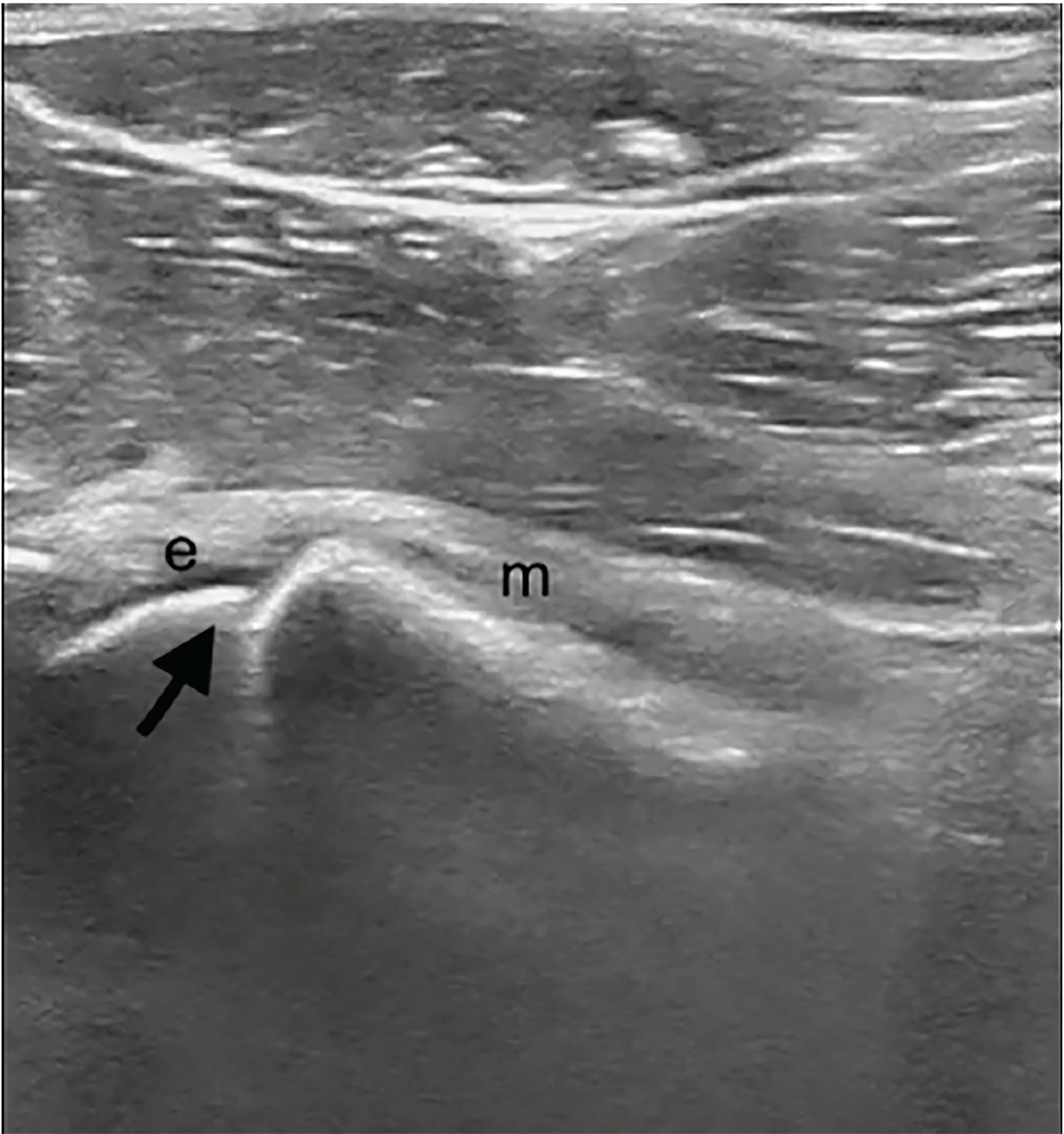
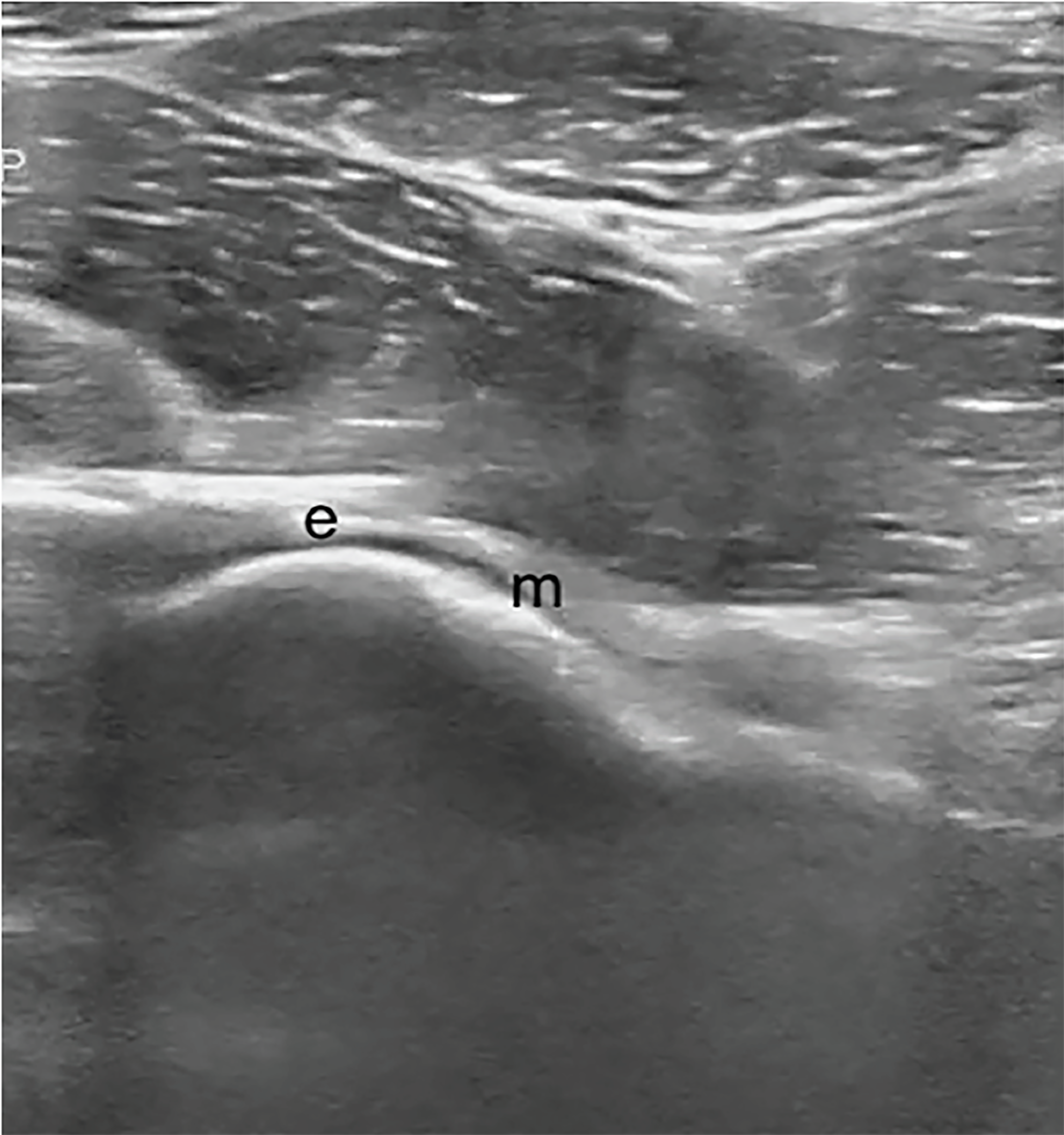
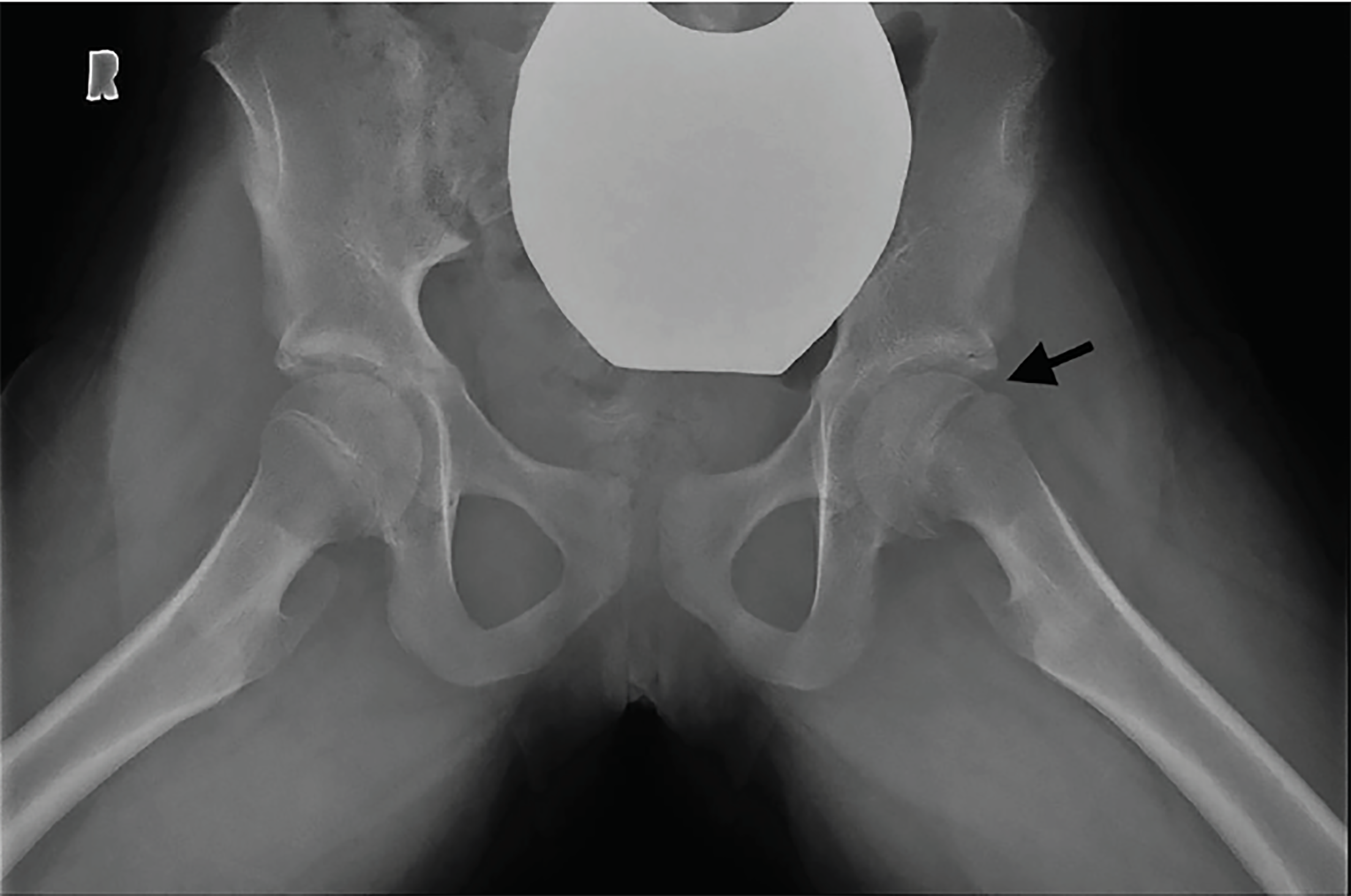
An 11-year-old female was brought to the emergency department with left hip and knee pain as well as limping for three weeks. There was no fever or recent trauma. Physical examination revealed restricted range of movement due to pain on hip flexion, internal and external rotation. A point-of-care ultrasound (POCUS) performed by an emergency physician (Image 1) raised the suspicion for her diagnosis when compared with right side (Image 2), which prompted expedited immobilization and pain control. POCUS was performed using a linear, high-frequency probe (14–5 MegaHertz) aligned parallel to the femoral neck. Subsequently, her pelvic radiograph (Image 3) confirmed the diagnosis.
DISCUSSION
Slipped capital femoral epiphysis (SCFE) is an important hip disorder of adolescence commonly occurring between the ages of 8–15 years. SCFE is characterized by a displacement of the capital femoral epiphysis from the metaphysis (femoral neck), through the growth plate.1 SCFE usually presents with sudden or progressive limping with hip, groin, thigh or even knee pain.1 Delayed diagnosis has been associated with increased severity of slip and complications, including avascular necrosis of the femoral head, chondrolysis and osteoarthritis.2
Although plain radiographs are the primary modality used to diagnose SCFE, ultrasound has also been used for diagnosis, staging and follow-up management of SCFE.3 Key ultrasound findings include posterior displacement of epiphysis with a physeal step, reduced distance between the anterior rim of the acetabulum and the metaphysis, remodeling of the metaphysis and, occasionally, joint effusion.4 Ultrasound sensitivity in diagnosis of SCFE is as high as 95%3, Its point-of-care use by emergency physicians can be a useful adjunct as a non-radiating, readily available bedside modality for assessing the limping child – especially in low-resource or rural settings where radiography may not be readily available or would require subsequent transfer to a different facility.
The patient underwent open reduction and internal fixation with uneventful recovery.
CPC-EM Capsule
What do we already know about this clinical entity?
Slipped capital femoral epiphysis (SCFE) is a disorder of older children and adolescents presenting with progressive unilateral pain and limp.
What is the major impact of the image(s)?
These images demonstrate sonographic findings of SCFE, particularly epiphyseal displacement from metaphysis of femur when compared with unaffected side.
How might this improve emergency medicine practice?
Point-of-care ultrasound provides a rapid, non-ionizing bedside method to diagnose SCFE, allowing early immobilization, pain control and expedited management in the emergency department.
Footnotes
Section Editor: Rick A. McPheeters, DO
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
Documented patient informed consent and/or Institutional Review Board approval has been obtained and filed for publication of this case report.
Address for Correspondence: Imran Asad, MD, University of Toronto, Hospital for Sick Children, Division of Pediatric Emergency Medicine, Department of Pediatrics, 555 University Avenue, Toronto, ON, Canada M5G1X8. Email: Imran.asad@sickkids.ca. 3:81 – 82
Submission history: Revision received October 21, 2018; Submitted November 28, 2018; Accepted January 1, 2019
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Peck DM, Voss LM, Voss TT. Slipped capital femoral epiphysis: diagnosis and management. Am Fam Physician. 2017;95(12):779-84.
2. Rahme D, Comley A, Foster B, et al. Consequences of diagnostic delays in slipped capital femoral epiphysis. J Pediatr Orthop B. 2006;15(2):93-7.
3. Magnano GM, Lucigrai G, De Filippi C, et al. Diagnostic imaging of the early slipped capital femoral epiphysis. Radiol Med. 1998;95(1–2):16-20.
4. Palaniappan M, Indiran V, Maduraimuthu P. Ultrasonographic diagnosis of slipped capital femoral epiphysis. Pol J Radiol. 2017;82:149-51.