
{kind=link}
| Author | Affiliation |
|---|---|
| Michael Lee, MD, JD | Boston Children’s Hospital, Division of Emergency Medicine, Boston, Massachusetts |
| Michael George, MD | Boston Children’s Hospital, Division of Radiology, Boston, Massachusetts |
| Kate E. Dorney, MD | Boston Children’s Hospital, Division of Emergency Medicine, Boston, Massachusetts |
Case presentation
Case discussion
ABSTRACT
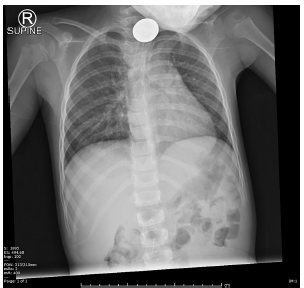
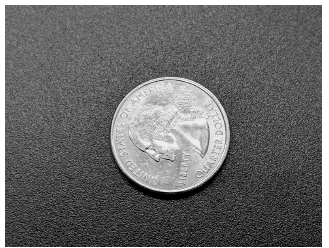
A four-year-old girl presented to the emergency department vomiting after a foreign body ingestion. An anteroposterior plain radiograph demonstrated a disc-shaped foreign body. Ordinarily, a plain radiograph cannot conclusively identify an object as a coin rather than a button battery that requires emergent removal. However, this high-voltage radiograph, windowed to increase contrast, showed the visible face of George Washington to confirm the diagnosis of an ingested quarter.
CASE PRESENTATION
A four-year-old girl presented to the emergency department with several episodes of vomiting; on questioning, she stated that she had swallowed something at daycare. Her parents were unsure whether she had access to button batteries. She had no respiratory distress on physical exam. The hospital obtained a single plain radiograph, an anteroposterior (AP) view of the chest (Image 1), and referred her to our tertiary center. The patient had no lateral film, but on high-contrast windowing of the film, which had been taken at a peak kilovoltage (kVp) of 100, the visible face of George Washington identified the object as a quarter (Images 2 and 3). The quarter was removed endoscopically without complication.

CASE DISCUSSION
In a disc-shaped foreign body ingestion, identifying the foreign body is critical but can be challenging. Esophageal button batteries must be removed emergently, given the high risk of injury, while an esophageal coin can be removed urgently unless the patient cannot manage her secretions.1 On radiographs, a double halo on the AP view or a step-off seen on a lateral view suggests that a round object is likely to be a button battery.1 Although the location cannot be definitively determined without a lateral film, an object seen en face in the AP view is more likely to be esophageal than tracheal.2,3 Additionally, our patient’s symptoms – vomiting and dysphagia without respiratory distress – suggested an esophageal location.
In our patient, the unusual visibility of George Washington’s face was possible because the image was acquired at 100 kVp, at the higher end of the dose range for patients of this age and size. While somewhat reducing subject contrast, this voltage allowed the beam to better penetrate metal and therefore enhanced the clarity of the quarter while delivering a lower radiation dose to the patient.4
CPC-EM Capsule
What do we already know about this clinical entity?
When a disc-shaped foreign body is seen on a plain radiograph, differentiating between coins and button batteries is critical but can be challenging.
What is the major impact of the image(s)?
The attached radiograph, taken at a peak kilovoltage (kVp) of 100, demonstrated the visible face of George Washington, identifying the object as a quarter.
How might this improve emergency medicine practice?
kVp doses at the high end of the range for a patient’s age and weight and high-contrast windowing, may help identify metallic foreign bodies.
Footnotes
Section Editor: Rick A. McPheeters, DO
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
Documented patient informed consent and/or Institutional Review Board approval has been obtained and filed for publication of this case report.
Address for Correspondence: Michael Lee, Jr., MD, JD, Boston Children’s Hospital, Division of Emergency Medicine, 300 Longwood Ave., Boston, MA 02215. Email: michael.lee@childrens.harvard.edu. 3:174 – 175
Submission history: Revision received November 30, 2018; Submitted January 24, 2019; Accepted January 30, 2019
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Kramer RE, Lerner DG, Lin T, et al. Management of ingested foreign bodies in children: a clinical report of the NASPGHAN Endoscopy Committee. J Pediatr Gastroenterol Nutr. 2015;60(4):562-74.
2. Raney LH, Losek JD. Esophageal coin and atypical radiograph. Pediatr Emerg Care. 2008;24(9):645-6.
3. Conners GP, Hadley JA. Esophageal coin with an unusual radiographic appearance. Pediatr Emerg Care. 2005;21(10):667-9.
4. Bushberg JT, Seibert JA, Leidholdt EM, et al. The Essential Physics of Medical Imaging. 2002.