
{kind=link}
| Author | Affiliation |
|---|---|
| Malia J. Moore, MD | Carl R. Darnall Army Medical Center, Department of Emergency Medicine, Fort Hood, Texas |
| Sophia Y. Liu, MD | Carl R. Darnall Army Medical Center, Department of Emergency Medicine, Fort Hood, Texas |
ABSTRACT
Fat embolism (FE) is a classically taught complication of long bone fractures, with the potential to cause high morbidity and mortality; however, it is rarely apparent on emergency department (ED) presentation or imaging. If recognized by the ED clinician, development of symptoms of FE may be avoided by early surgical fixation and potentially by corticosteroid administration.
CASE PRESENTATION
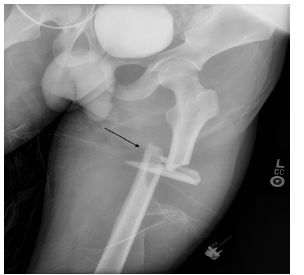
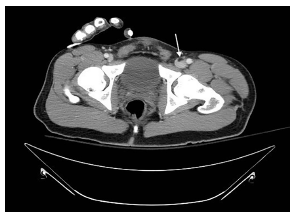
The patient was an adult male involved in a high-speed motor vehicle collision into a tree, with prolonged extrication due to vehicle deformity. On initial trauma exam, he had obvious left femur and left wrist deformities. A radiograph of the left hip revealed a femur fracture (Image 1). Computed tomography (CT) of the head, spine, chest, abdomen, and pelvis were performed. Imaging identified a fat embolism (FE) in the left common femoral vein (Images 2 and 3).

DISCUSSION
CT images showed a fat fluid level within the left common femoral vein as a direct complication of femur fracture. FE is a rare syndrome in which fat globules migrate into vasculature, most commonly from traumatized adipose tissue or marrow-containing bone. FE can complicate a wide variety of conditions, most commonly long bone or pelvic fractures. Symptomatic fat emboli present with a triad of hypoxemia, neurologic abnormality, and petechial rash. Although care is largely supportive, the patient should be carefully monitored with pulse oximetry, frequent neurologic checks, and re-examination to promptly identify and treat development of FE syndrome. All symptoms are transient if not fatal.1,2
Early recognition of FE may prompt steps to avoid development of the clinical syndrome, such as early surgical fixation, which is preferred over traction, and corticosteroid administration. Corticosteroids have shown some benefit, especially in high-risk injuries with confirmed fat emboli; however, their routine empiric administration is controversial.3-5
CPC-EM Capsule
What do we already know about this clinical entity?
Fat embolism (FE), a condition in which fat globules migrate into vasculature, is a known complication of long bone fractures that could lead to the development of FE syndrome.
What is the major impact of the image(s)?
The asymptomatic finding of FE in transit shown here is believed to be rare; however, its identification could help avoid the development of FE syndrome.
How might this improve emergency medicine practice?
Early identification of FE may prompt treatment and lessen the risk of morbidity and mortality associated with FE syndrome.
Footnotes
Section Editor: Anna McFarlin, MD
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
Documented patient informed consent and/or Institutional Review Board approval has been obtained and filed for publication of this case report.
Address for Correspondence: Malia J. Moore, MD, Carl R. Darnall Army Medical Center, Department of Emergency Medicine, 36065 Santa Fe Drive, Fort Hood, TX 76544. Email: majmoore@gmail.com. 3:176 – 177
Submission history: Revision received December 3, 2018; Submitted February 5, 2019; Accepted February 8, 2019
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none. The views expressed here are those of the authors and do not reflect the official policy of the Department of the Army, the Department of Defense, or the US Government.
REFERENCES
1. Shaikh N. Emergency management of fat embolism syndrome. J Emerg Trauma Shock. 2009;2(1):29-33.
2. Kosova E, Bergmark B, Piazza G. Fat embolism syndrome. Circulation. 2015;131(3):317-20.
3. Schonfeld SA, Ploysongsang Y, DiLisio R, et al. Fat embolism prophylaxis with corticosteroids. A prospective study in high-risk patients. Ann Intern Med. 1983;99(4):438-43.
4. Bederman SS, Bhandari M, McKee MD, et al. Do corticosteroids reduce the risk of fat embolism syndrome in patients with long-bone fractures? A meta-analysis. Can J Surg. 2009;52(5):386-93.
5. Sen RK, Tripathy SK, Krishnan V. Role of corticosteroid as a prophylactic measure in fat embolism syndrome: a literature review. Musculoskelet Surg. 2012;96(1):1-8.