
{kind=link}
| Author | Affiliation |
|---|---|
| Emily Fite, MD | Saint Louis University School of Medicine, Saint Louis, Missouri |
| Jennifer Fitzgerald, BS | Saint Louis University School of Medicine, Saint Louis, Missouri |
| Quinn Kistenfeger, BS | Saint Louis University School of Medicine, Division of Emergency Medicine, Department of Surgery, Saint Louis, Missouri |
ABSTRACT
A 27-year-old female presented to the emergency department with fevers, nausea, chills, and non-specific bilateral lower quadrant abdominal pain. A pregnancy test was negative. Computed tomography demonstrated moderate left hydronephrosis secondary to tubo-ovarian abscess (TOA). The abscess was so large it distorted local anatomy and compressed the ureters. She was prescribed merepenem and admitted for care by obstetrics/gynecology.
CASE PRESENTATION
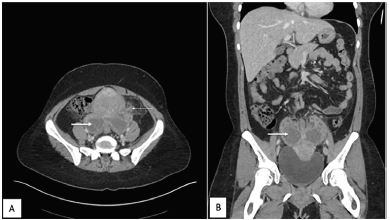
A 27-year-old female presented to the emergency department with bilateral lower quadrant abdominal pain, fever, nausea, chills, and body aches. She stated she had been ill for three days and was getting worse. She was vomiting all oral intake and had new vaginal discharge. Upon examination, she was febrile to 101.1° Fahrenheit with a heart rate of 160 beats per minute. Her pregnancy test was negative. She had voluntary guarding and generalized tenderness on her abdominal exam while pelvic exam revealed cervical motion tenderness with copious vaginal discharge. Patient was given fluids and pain medication, and we obtained computed tomography (CT) of the abdomen and the pelvis with intravenous contrast (Images 1 and 2).

DISCUSSION
This case demonstrates the complications that can occur when pelvic inflammatory disease goes untreated. Tubo-ovarian abscesses (TOA) can form from an ascending infection of the female genital tract leaking purulent discharge through the fallopian tube and forming a pus-filled mass encompassing the tube and/or ovary.1 In this case, the abscess was so large that it distorted local anatomy and compressed the ureters, causing hydronephrosis. Ultrasonography or CT can be used to evaluate nonspecific symptoms and look for specific complications associated with pelvic inflammatory disease.2 The CT demonstrated findings consistent with the presence of a TOA with hydronephrosis (Image 2).
First-line treatment of TOA with broad-spectrum antibiotics should begin immediately after blood cultures are taken.1 Treatment with antibiotics has been shown to be effective in many patients, but recurrence is likely. Surgical intervention may be considered if it is a recurrence, nonresponsive to antibiotics, or if rupture occurs.1,3 Minimally invasive measures should be considered, especially in women of childbearing age, to avoid causing infertility.3 Our patient was prescribed meropenem and she was admitted for care by her obstetrician-gynecologist.
CPC-EM Capsule
What do we already know about this clinical entity?
Untreated tubo-ovarian abscess (TOA) can lead to abscess rupture, sepsis, and infection of nearby organs.
What is the major impact of the image(s)?
In our case, the patient had a TOA so large that it put pressure on the ureters, causing bilateral hydronephrosis.
How might this improve emergency medicine practice?
TOA is a less common diagnosis. Treatment should begin promptly with broad-spectrum antibiotics and may require surgical intervention to prevent abscess rupture and sepsis.
Footnotes
Section Editor: Rick A. McPheters, DO
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
Documented patient informed consent and/or Institutional Review Board approval has been obtained and filed for publication of this case report.
Address for Correspondence: Quinn Kistenfeger, BS, Saint Louis University School of Medicine, Address, Saint Louis, MO 63110. Email: quinn.kistenfeger@health.slu.edu. 4:92 – 93
Submission history: Revision received July 16, 2019; Submitted November 1, 2019; Accepted October 17, 2019
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Munro K, Gharaibeh A, Nagabushanam S, et al. Diagnosis and management of tubo-ovarian abscesses. Obstet Gynecol. 2018;20(1):11-9.
2. Rezvani M, Shaaban AM. Fallopian tube disease in the nonpregnant patient. Radiographics. 2011;31(2):527-48.
3. Tokumaru T, Shima Y, Okabayashi T, et al. Emergency surgery for tubo-ovarian abscess identified extended-spectrum beta-lactamase-producing : the first case presentation revealing causative bacteria. Surg Case Rep. 2015;1(1):66.