
{kind=link}
| Author | Affiliation |
|---|---|
| Júlio C. Garcia de Alencar, MD | São Paulo University, Department of Emergency Medicine, São Paulo, Brazil |
| Millena G. Pinheiro Costa, MD | São Paulo University, Department of Emergency Medicine, São Paulo, Brazil |
| Rodrigo A. Brandao Neto, PhD | São Paulo University, Department of Emergency Medicine, São Paulo, Brazil |
| Heraldo Possolo de Souza, PhD | São Paulo University, Department of Emergency Medicine, São Paulo, Brazil |
ABSTRACT
Pigtail catheters have emerged as an effective and less morbid alternative to traditional chest tubes for evacuation of pleural air. Rare complications in the literature have been reported. We report a case of a 92-year-old male who presented with dyspnea and shock, noted to have a pneumothorax requiring tube thoracostomy. Computed tomography demonstrated pigtail within the lung parenchyma. We discuss the implications of this occurrence.
CASE PRESENTATION
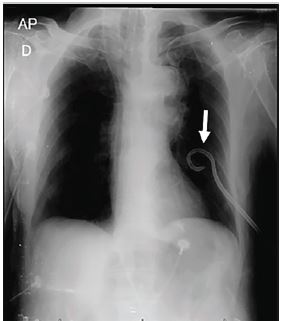
A 92-year-old male presented to the emergency department with a 4-day history of flu-like symptoms and shortness of breath that had progressed to respiratory failure. On admission, he was intubated and on vasopressors due to circulatory shock. Endotracheal intubation had been performed at an outside facility; mechanical ventilation was reportedly difficult. At examination, no breath sounds were audible on the left side, and the jugular veins were distended. Point-of-care ultrasound showed no lung sliding on the left. Tube thoracostomy was performed and a pigtail catheter placed, with positive air drainage. Chest radiograph showed a well-positioned catheter and good lung expansion (Image 1).
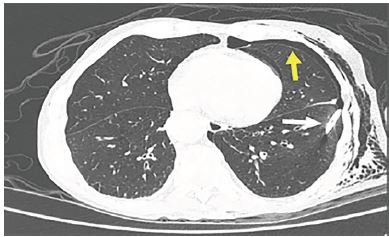
On day two, the patient was extubated and transferred to the Intermediate Care Unit. Three days later he had abrupt onset of dyspnea, extensive subcutaneous emphysema, and drainage of serosanguinous fluid through the chest tube instead of air. Chest computerized tomography showed the pigtail within the lung parenchyma and a residual pneumothorax (Image 2).
The decision was to remove the pigtail and place a traditional chest tube. The patient had an uneventful course, with complete resolution of pneumothorax. The chest tube was removed after six days, and the patient was discharged without further complications.
DISCUSSION
Pigtail catheters offer reliable treatment of pneumothoraces, and are a safe and less invasive alternative to tube thoracostomy.1 Rare complications in the literature such as intraparenchymal insertion, left ventricular penetration, subclavian artery laceration and cerebral air embolism have been reported.2 Image guided technique, ideally ultrasound, should be utilized for pig tail insertion to minimize the risk of complications.3
CPC-EM Capsule
What do we already know about this clinical entity?
Pigtail catheters offer reliable treatment of pneumothoraces, and are a safe and less invasive alternative to tube thoracostomy. Rare complications have been reported.
What is the major impact of the image(s)?
We discuss the implications of this occurrence and recommended management based on our experience.
How might this improve emergency medicine practice?
Image guided technique, ideally ultrasound point-of-care, should be utilized for pigtail insertion to minimize the risk of complications.
Footnotes
Section Editor: Rick A. McPheeters, DO
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
Documented patient informed consent and/or Institutional Review Board approval has been obtained and filed for publication of this case report.
Address for Correspondence: Júlio C. Garcia de Alencar, MD, São Paulo University, Deparment of Emergency Medicine, 255 Eneas de Carvalho Aguir, São Paulo, Brazil 05403-000. Email: julio.alencar@hc.fm.usp.br. 4:90 – 91
Submission history: Revision received August 19, 2019; Submitted October 25, 2019; Accepted November 11, 2019
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Gammie JS, Banks MC, Fuhrman CR, et al. The pigtail catheter for pleural drainage: a less invasive alternative to tube thocatostomy. JSLS. 1999;3(1):57-61.
2. Saqib A, Ibrahim U, Maroun R. An unusual complication of pigtail catheter insertion. J Thoracic Dis. 2018;10(10):5964-7.
3. Laws D, Neville E, Duffy J. Pleural diseases group, standards of care committee, British Thoracic Society: BTS guidelines for the insertion of a chest drain. Thorax. 2003;58(suppl 2):53-9.