
{kind=link}
| Author | Affiliation |
|---|---|
| Dawa Sherpa, MD | Alameda Health System – Highland Hospital, Oakland, California |
| Brian D. Johnson, MD, MPH | University of Washington – Valley Medical Center, Renton, Washington |
| Leila Ben-Youssef, MD, MA | Alameda Health System – Highland Hospital, Oakland, California |
| Arun Nagdev, MD | Alameda Health System – Highland Hospital, Oakland, California; University of California, San Francisco, San Francisco, California |
CASE PRESENTATION
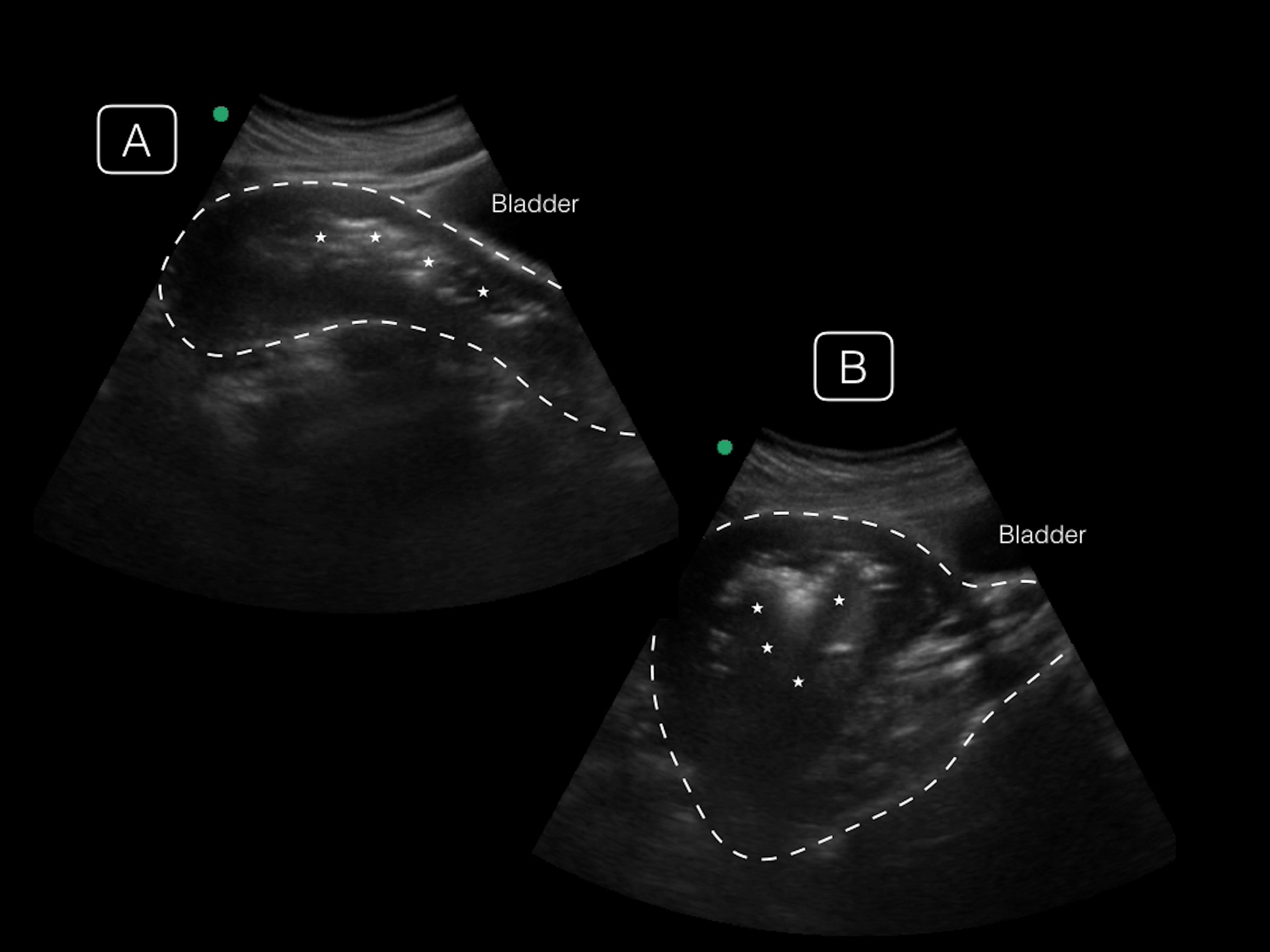
A 19-year-old recently immigrated female presented with severe lower abdominal pain, fever, and vaginal bleeding after a syncopal episode. On examination, she was febrile with diffuse tenderness to palpation of her lower abdomen with an enlarged uterus palpable to just below the umbilicus. The patient initially denied pregnancy, but had a positive urine pregnancy with a quantitative beta-human chorionic gonadotropin of 19,773 mIU/mL. Pelvic exam revealed scant amount of blood in the vaginal canal with malodorous discharge. A point-of-care ultrasound revealed an enlarged uterus with a large amount of air and echogenic debris within the endometrium (Image). Over the course of the emergency department (ED) stay, the patient became hypotensive and was found to have anemia and leukocytosis requiring a blood transfusion, antibiotics and emergent gynecological intervention.
DISCUSSION
The patient was admitted to the obstetric service and started on broad-spectrum antibiotics for incomplete septic abortion. She underwent a vacuum-assisted dilation and curettage with removal of uterine contents. Surgical pathology revealed degenerating and focal necrotic chorionic villi consistent with intra-uterine pregnancy. While rare in developed countries, septic abortion is a life-threatening infection of the placenta and fetus of a previable pregnancy typically associated with unsafe abortion practices.1 Diagnosis is made clinically and confirmed by ultrasound, computed tomography or magnetic resonance imaging that can show an enlarged uterus with hemorrhage, retained intrauterine material, free fluid, abscess formation and/or air. 2 Intrauterine air is theorized to arise from gas-forming organisms or secondary to perforation from unsafe abortion practices. The ultrasonographic finding of air in the uterus must be recognized by the emergency physician in order to expedite ED and consultative care. With the reduction in funding for healthcare services for at-risk populations and possible defunding of Planned Parenthood, we believe that this uncommon finding may become more prevalent for providers on the front line.4,5 Treatment consists of broad-spectrum antibiotics, prompt removal of infected tissue and hysterectomy in severe, refractory cases.3
CPC-EM Capsule
What do we already know about this clinical entity?
Septic abortion is a life-threatening infection associated with unsafe abortion practices that is diagnosed clinically and confirmed with ultrasound.
What is the major impact of the image(s)?
Our ultrasound video demonstrates septic abortion-associated uterine free air, a novel finding that has yet to be discussed in the point-of-care ultrasound (POCUS) emergency medicine literature.
How might this improve emergency medicine practice?
POCUS allows for prompt identification of septic abortion and swift consultation with obstetrics for definitive care.
Footnotes
Section Editor: Rick A. McPheeters, DO
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
Address for Correspondence: Dawa Sherpa, MD, Highland Hospital – Alameda Health System, 1411 East 31st Street, Oakland, CA 94602. Email: dsherpa@alamedahealthsystem.org. 1:268 – 269
Submission history: Revision received January 11, 2017; Submitted March 1, 2017; Accepted March 31, 2017
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Unsafe abortion – global and regional estimates of the incidence of unsafe abortion and associated mortality in 2008. 2011:1-66.
2. Saultes TA, Devita D, Heiner JD. The back alley revisited: sepsis after attempted self-induced abortion. West J Emerg Med. 2009;10(4):278-80.
3. Stubblefield PG, Grimes DA. Septic abortion. N Engl J Med. 1994;331(5):310-4.
4. The Mexico City Policy – Memorandum for the Secretary of State[,] the Secretary of Health and Human Services[, and] the Administrator of the United States Agency for International Development. Federal Register. 2017.
5. Sengupta Somini. Trump Revives Ban on Foreign Aid to Groups That Give Abortion Counseling. The New York Times. 2017 Accessed January 24, 2017.
SUPPLEMENTARY MATERIAL
Transabdominal ultrasound of the uterus with debris and air with shadowing artifact.