
{kind=link}
| Author | Affiliation |
|---|---|
| Justin Yanuck, MD, MS | University of California, Irvine, Department of Emergency Medicine, Irvine, California |
| Ghadi Ghanem, | University of California, Irvine, Department of Emergency Medicine, Irvine, California |
| Shadi Lahham, MD, MS | University of California, Irvine, Department of Emergency Medicine, Irvine, California |
CASE PRESENTATION
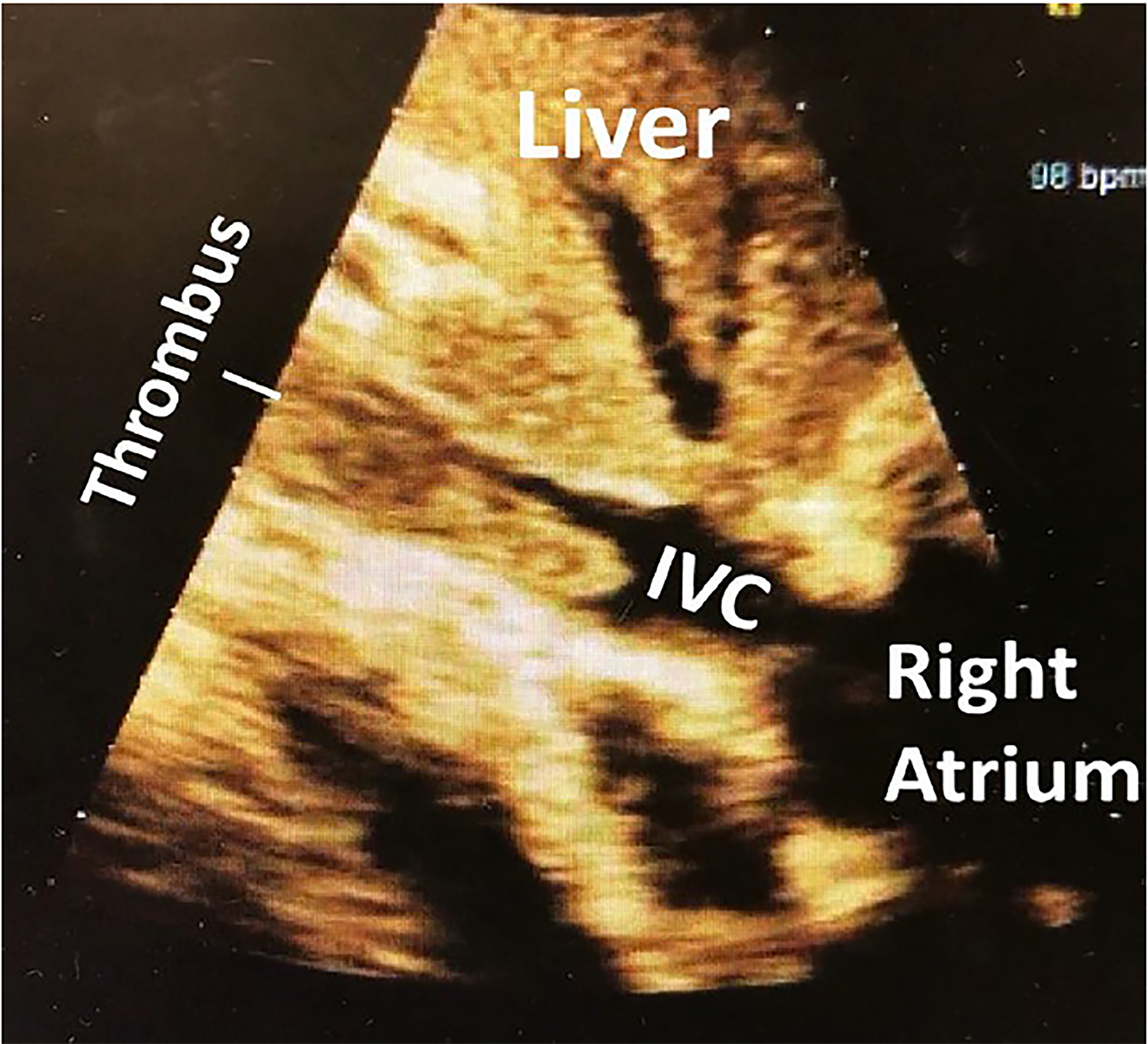
A 74-year-old male with a history of metastatic prostate cancer presented to the emergency department with hypotension and shortness of breath. We assessed volume status using point-of-care ultrasound (POCUS) with a phased array probe in the subxiphoid orientation. This revealed a large inferior vena cava (IVC) thrombus extending from above the IVC bifurcation into the right atrium (Image, Video). The patient was started on intravenous heparin and fluids. Computed tomography (CT) pulmonary angiogram revealed an occlusive pulmonary embolism (PE) in the right lower lobe.
DISCUSSION
Venous thromboembolisms are estimated to occur in 0.1% of patients; 1.5% of patients hospitalized with deep vein thrombosis (DVT) were diagnosed with vena cava thrombosis, of whom 12% had a pulmonary embolism.1,2 The mortality rate for IVC thrombosis patients is nearly double that of DVT patients.1,3 These patients can present with lower limb swelling or pain, lower back pain, fever, or elevated inflammatory markers.3 CT or magnetic resonance imaging is often used to make the diagnosis.4,5
Recently, ultrasound has shown promise for quick identification of IVC thrombus.6 The rapid ultrasound for shock and hypotension (RUSH) protocol, which incorporates assessment of IVC intravascular volume status, can be used for these undifferentiated patients to diagnose conditions not apparent with the standard physical exam.7,8 The RUSH examination led to the definitive diagnosis and etiology of this patient’s hypotension and dyspnea.
Once diagnosed, confirmation using CT imaging and admission to the hospital for anticoagulation and hemodynamic monitoring is recommended.9 Invasive treatments include angioplasty or local thrombolysis.3
Our case highlights the use of POCUS to quickly identify etiologies of hypotensive and dyspneic patients. Further imaging should be obtained in IVC thrombosis patients to rule out PE or additional clots.
CPC-EM Capsule
What do we already know about this clinical entity?
Inferior vena cava thrombosis is a rare, life-threatening condition that usually requires advanced imaging techniques to diagnose.
What is the major impact of the image(s)?
This image highlights the utility of the rapid ultrasound for shock and hypotension protocol for finding both obvious and less-obvious pathologies.
How might this improve emergency medicine practice?
Rapid diagnosis of undifferentiated hypotensive patients using point-of-care ultrasound expedites care and medical intervention.
Footnotes
Section Editor: Scott Goldstein, DO
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
Documented patient informed consent and/or Institutional Review Board approval has been obtained and filed for publication of this case report.
Address for Correspondence: Justin Yanuck, MD, MS, University of California, Irvine, Department of Emergency Medicine, 333 City Blvd. West, Suite 640, Orange, CA 92868. Email: jyanuck@uci.edu. 3:67 – 68
Submission history: Revision received September 23, 2018; Submitted November 23, 2018; Accepted January 1, 2019
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. White RH. The epidemiology of venous thromboembolism. Circulation. 2003;107(23 Suppl 1):I4-8.
2. Stein PD, Matta F, Yaekoub AY. Incidence of vena cava thrombosis in the United States. Am J Cardiol. 2008;102(7):927-9.
3. McAree B, O’Donnell M, Fitzmaurice G, et al. Inferior vena cava thrombosis: a review of current practice. Vasc Med. 2013;18(1):32-43.
4. Soler R, Rodríguez E, López MF, et al. MR imaging in inferior vena cava thrombosis. Eur J Radiol. 1995;19(2):101-7.
5. Giordano P, Weber K, Davis M, et al. Acute thrombosis of the inferior vena cava. Am J Emerg Med. 2006;24(5):640-2.
6. Lahham S, Tsai L, Wilson SP, et al. Thrombosis of inferior vena cava diagnosed using point-of-care ultrasound after pediatric near-syncope. J Emerg Med. 2016;51(4):e89-91.
7. Jones AE, Tayal VS, Sullivan DM, et al. Randomized, controlled trial of immediate versus delayed goal-directed ultrasound to identify the cause of nontraumatic hypotension in emergency department patients. Crit Care Med. 2004;32(8):1703-8.
8. Perera P, Mailhot T, Riley D, et al. The RUSH exam: rapid ultrasound in shock in the evaluation of the critically ill. Emerg Med Clin North Am. 2010;28(1):29-56.
9. Kearon C, Akl EA, Comerota AJ, et al. Antithrombotic therapy for VTE disease: antithrombotic therapy and prevention of hrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2):e419S-96S.
SUPPLEMENTARY MATERIAL
Rapid ultrasound for shock and hypotension protocol using the phased array probe in the subxiphoid orientation revealed a large thrombus situated in the inferior vena cava.