
{kind=link}
| Author | Affiliation |
|---|---|
| Christopher Parker, DO | University of Illinois College of Medicine, Department of Emergency Medicine, Chicago, Illinois |
| Wesley Eilbert, MD | University of Illinois College of Medicine, Department of Emergency Medicine, Chicago, Illinois |
| Timothy Meehan, MD | University of Illinois College of Medicine, Department of Emergency Medicine, Chicago, Illinois |
| Christopher Colbert, DO | University of Illinois College of Medicine, Department of Emergency Medicine, Chicago, Illinois |
Introduction
Case report
Discussion
Conclusion
ABSTRACT
Colpocephaly is a form of congenital ventriculomegaly characterized by enlarged occipital horns of the lateral ventricles with associated neurologic abnormalities. The diagnosis of colpocephaly is typically made in infancy. Its diagnosis in adulthood without associated clinical symptoms is exceptionally rare. We report a case of colpocephaly diagnosed incidentally in an adult without neurologic abnormalities in the emergency department. To our knowledge, this is only the ninth reported case in an asymptomatic adult and the first to be described in the emergency medicine literature.
INTRODUCTION
Colpocephaly is a rare form of congenital ventriculomegaly often associated with partial or complete agenesis of the corpus callosum. Diagnosis is typically made in infancy due to associated neurological and neurodevelopmental disorders.1,2 Initial discovery in adulthood is exceedingly rare.3-9 When identified incidentally in adults, colpocephaly may be misdiagnosed as hydrocephalus.4,7,9 We report a case of colpocephaly in an adult of normal neurological development discovered in the emergency department (ED).
CASE REPORT
A 29-year-old male with no pertinent past medical history presented to our ED with two weeks of intermittent headaches. His headache was described as throbbing in character, localized to the bitemporal region, non-radiating, and non-positional. The headache occurred daily, lasting a few minutes to hours, with no particular exacerbating factors. His symptoms improved with acetaminophen, which he used sparingly. He reported no associated vomiting, gait abnormalities, vision changes, confusion, urinary changes, or other neurologic abnormalities. He had been treated at four different EDs in the two weeks prior to presentation for the headaches, but no imaging studies had been performed. The patient had no psychiatric history. His highest level of education was a high school diploma, and he was unemployed.
On arrival, the patient was afebrile with pulse, blood pressure, and respiratory rate all within the normal range. Physical examination revealed an anxious male who was alert, oriented, and in no acute distress. His head was normocephalic with no evidence of trauma. His pupils were equal, round, and reactive to light. His neurological examination did not reveal any cranial nerve deficits, speech abnormalities, muscle weakness, or loss of sensation. His reflexes were intact and symmetrical. His coordination was normal. His gait was stable with balanced cadence, and he exhibited a negative Romberg test. His visual acuity was 20/20 in both eyes. The remainder of the examination was unremarkable.
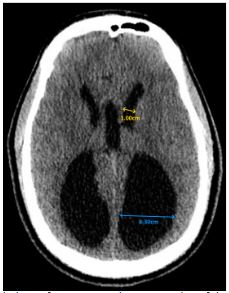
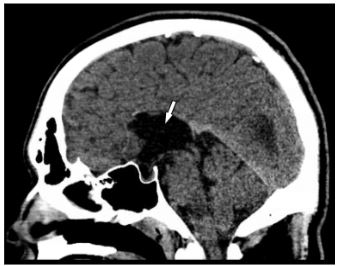
Laboratory values of complete blood count and complete metabolic panel were unremarkable. The serum carboxyhemoglobin level was within the normal range. Due to the patient’s headache not being fully consistent with a primary headache and his multiple visits to the ED without a history of imaging, computed tomography (CT) of the head was ordered to assess for a possible anatomic cause of his symptoms. The CT was notable for marked enlargement of the occipital horns of the lateral ventricles with agenesis of the corpus callosum, consistent with colpocephaly (Images 1 and 2).
The patient was evaluated by the neurology service in the ED. It was their opinion that his headaches were primary in nature and not associated with the incidental finding of colpocephaly. His headache resolved after receiving 10 milligrams (mg) of intravenous metoclopramide and 50 mg of oral diphenhydramine, and he was discharged home with neurology follow-up. The patient returned to the ED one month later for an unrelated complaint and did not report a headache at that time.
CPC-EM Capsule
What do we already know about this clinical entity?
Colpocephaly is a congenital form of ventriculomegaly. Diagnosis is typically made in infancy due to associated neurologic abnormalities.
What makes this presentation of disease reportable?
This is only the ninth reported case of colpocephaly diagnosed in an asymtomatic adult and the first to be described in the emergency medicine literature.
What is the major learning point?
While exceptionally rare, colpocephaly may be present in asymptomatic adults. It may be misdiagnosed in adults as normal pressure hydrocephalus.
How might this improve emergency medicine practice?
Knowledge of the clinical and radiographic differences between colpocephaly and normal pressure hydrocephalus will help avoid unnecessary diagnostic and therapeutic procedures.
DISCUSSION
First described by Benda in 1940, colpocephaly is a rare congenital brain malformation in which the occipital horns are disproportionately larger than the anterior horns of the lateral ventricles.10 Colpocephaly can be associated with partial or complete agenesis of the corpus callosum, Chiari malformations, lissencephaly, and microcephaly.9 The abnormal ventricular enlargement in colpocephaly is believed to be secondary to the developmental arrest of white matter formation that occurs during fetal development.7 Various etiologies have been proposed, including chromosomal abnormalities, intrauterine infection, perinatal anoxic-ischemic encephalopathy, intrauterine growth retardation, and maternal toxin exposure.1,3
Colpocephaly is typically discovered in infancy due to associated intellectual disability, seizures, motor abnormalities, or visual abnormalities.1,2 Discovery in adulthood is remarkably uncommon and has only been reported eight times previously (Table 1).3-9 Colpocephaly can be identified radiographically by measuring the maximal width of the anterior and occipital horns of the lateral ventricles. An occipital-to-anterior horn ratio of greater than 3 is highly specific for colpocephaly, although it has relatively low sensitivity.3,11
| Author | Year | Patient | Reason for imaging |
|---|---|---|---|
| Wunderlich G, et al.6 | 1996 | 60-year-old female | New onset partial complex seizures |
| Cheong J, et al.7 | 2012 | 67-year-old female | Four months of headache and dizziness – ultimately diagnosed with meningioma |
| Esenwa C, et al.3 | 2013 | 60-year-old female | Headache after minor head trauma |
| Ciurea R, et al.9 | 2014 | 28-year-old female | Longstanding, intermittent headaches and vertigo |
| Brescian N, et al.8 | 2014 | 88-year-old male | New onset left hand apraxia |
| Nasrat T, et al.4 | 2014 | 66-year-old female | One month of declining mental status – ultimately diagnosed with paraspinal abscess |
| Bartolome E, et al.5 | 2016 | 67-year-old female | Syncopal episode |
| 60-year-old female | Confusion with fever – ultimately diagnosed with an upper respiratory infection |
The identification of colpocephaly in adulthood is a phenomenon that has only recently been described. Colpocephaly discovered in adulthood may be misdiagnosed as normal pressure hydrocephalus, a much more common cause of ventriculomegaly in adults.3,5 Knowledge of the clinical and radiographic differences between these two conditions is needed to avoid unnecessary diagnostic and therapeutic procedures (Table 2). Colpocephaly discovered incidentally in asymptomatic adults requires no specific treatment.
| Colpocephaly | Normal pressure hydrocephaly3,12 | |
|---|---|---|
| Clinical characteristics | Typically diagnosed in infancy due to associated neurological abnormalities | Typically diagnosed after age 50 years |
| Diagnosis in asymptomatic adults is exceptionally rare | Symptoms include varying degrees of the classic triad of gait disturbance, urinary incontinence, and dementia | |
| Radiographic characteristics | Disproportionate dilation of the occipital horns of the lateral ventricles, often associated with full or partial agenesis of the corpus callosum | Ventriculomegaly marked by dilation of the anterior and occipital horns of the lateral ventricles |
| Treatment | No treatment is indicated when diagnosed in asymptomatic adults | CSF shunting procedures lead to symptom improvement in approximately 60% of cases |
CSF, cerebral spinal fluid.
CONCLUSION
Colpocephaly discovered in asymptomatic adults is exceedingly rare. It may be misdiagnosed as normal pressure hydrocephalus in the ED. It is important to differentiate between these two conditions to avoid unnecessary interventions.
Footnotes
Section Editor: Rick A. McPheeters, DO
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
Documented patient informed consent and/or Institutional Review Board approval has been obtained and filed for publication of this case report.
Address for Correspondence: Wesley Eilbert, MD, University of Illinois College of Medicine, Department of Emergency Medicine, 1819 West Polk St. Room 469 COME, Chicago, Illinois 60612. Email: weilbert@uic.edu. 3:421 – 424
Submission history: Revision received July 25, 2019; Submitted September 18, 2019; Accepted September 26, 2019
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Landman J, Weitz R, Dulitzki F, et al. Radiological colpocephaly: a congenital malformation or the result of intrauterine and perinatal brain damage. Brain Dev. 1989;11(5):313-6.
2. Herskowitz J, Rosman NP, Wheeler CB. Colpocephaly: clinical, radiologic, and pathogenetic aspects. Neurology. 1985;35(11):1594-8.
3. Esenwa CC, Leaf DE. Colpocephaly in adults. BMJ Case Rep. 2013;2013.
4. Nasrat T, Seraji-Bozoergzad N. Incidentally discovered colpocephaly and corpus callosum agenesis in an asymptomatic elderly patient. IJMBS. 2015;7(2):56-8.
5. Bartolome EL, Cottura JC, Britos Frescia R, et al. Asymptomatic colpocephaly and partial agenesis of corpus callosum. Neurologia. 2016;31(1):68-70.
6. Wunderlich G, Schlaug G, Jäncke L, et al. Adult-onset complex partial seizures as the presenting sign in colpocephaly: MRI and PET Correlates. J Neuroimaging. 1996;6(3):192-5.
7. Cheong JH, Kim CH, Yang MS, et al. Atypical meningioma in the posterior fossa associated with colpocephaly and agenesis of the corpus callosum. Acta Neurochir Suppl. 2012;113:161-71.
8. Brescian NE, Curiel RE, Gass CS. Case study: a patient with agenesis of the corpus callosum with minimal associated neuropsychological impairment. Neurocase. 2014;20(6):606-14.
9. Ciurea RB, Mihailescu G, Anton RM, et al. Corpus callosum dysgenesis and colpocephaly. Rom J Neurol. 2013;12(3):160-3.
10. Benda CE. Microcephaly. Am J Psychiatry. 1941;97(5):1135-46.
11. Noorani PA, Bodensteiner JB, Barnes PD. Colpocephaly: frequency and associated findings. J Child Neurol. 1988;3(2):100-4.
12. Shprecher D, Schwalb J, Kurlan R. Normal pressure hydrocephalus: diagnosis and treatment. Curr Neurol Neurosci Rep. 2008;8(5):371-6.