
{kind=link}
| Author | Affiliation |
|---|---|
| Stuart A. Ostby, MD | University of Alabama at Birmingham, Department of Obstetrics and Gynecology, Birmingham, Alabama |
| Michael Olushoga, MD | University of Alabama at Birmingham, Department of Emergency Medicine, Birmingham, Alabama |
| Charles A. Leath, MD | University of Alabama at Birmingham, Department of Obstetrics and Gynecology, Division of Gynecologic Oncology, Birmingham, Alabama |
| Samuel L. Burleson, MD | University of Alabama at Birmingham, Department of Emergency Medicine, Birmingham, Alabama |
ABSTRACT
Case Presentation
We describe the presentation to the emergency department of a patient with recurrent ovarian cancer treated with bevacizumab with the complication of bowel perforation.
Discussion
We review the frequency and outcomes of bevacizumab-related bowel perforation. We also report the patient’s imaging findings, including the radiologic presentation of free intraperitoneal air and portal venous gas, both indicative of bowel perforation and the need for emergent surgical evaluation. Our case also illustrates the potentially catastrophic side effects of bevacizumab and other targeted oncologic therapies of which emergecny physicians may not be aware.
CASE PRESENTATION
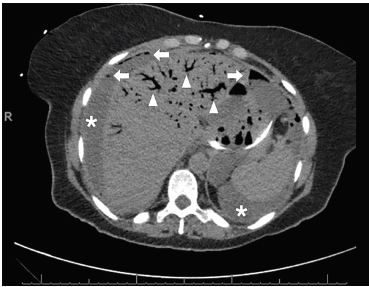
A 69-year-old, African-American female with recurrent stage IIIC ovarian carcinoma treated with bevacizumab presented to the emergency department (ED) with abdominal pain, distention, vomiting, and hypotension. After initial stabilization, an upright abdominal radiograph (Image 1) revealed peritoneal free air and portal venous gas concerning for bowel perforation, which was confirmed by computed tomography (CT) of the abdomen and pelvis (Images 2 and 3).


The patient was admitted to the gynecology oncology service and maintained on crystalloids and antibiotics. She had minimal symptoms. In accordance with her wishes, no further aggressive intervention was pursued, and she died on hospital day three.
DISCUSSION
Bevacizumab is a monoclonal antibody targeting the vascular endothelial growth factor receptor used in multiple cancer types, including ovarian.1, 2 Complications include bowel perforation and gastrointestinal (GI) bleeding.3 The incidence of bowel perforation in ovarian cancer treated with bevacizumab is estimated to be 2–3%,4 with a relative risk of 2.57 compared to ovarian cancer alone.5 Bowel perforation and other severe GI pathologies are seen with other commonly-used targeted therapies such as sunitinib, sorafenib, everolimus, and temsirolimus.6 This patient had other independent risk factors for perforation including bowel resection-reanastamosis, peritoneal carcinomatosis, and partial small bowel obstructions.
CPC-EM Capsule
What do we already know about this clinical entity?
Bevacizumab is an increasingly used targeted chemotherapeutic agent with infrequent, severe complications including gastrointestinal perforation.
What is the major impact of the image(s)?
Severe ischemic bowel related to bevacizumab therapy and widespread diagnostic findings of mesenteric ischemia, portal venous gas, and free air are demonstrated.
How might this improve emergency medicine practice?
Early recognition and diagnosis for bowel perforation in patients on bevacizumab is essential to allow prompt surgical evaluation and therapy.
Bowel perforation secondary to bevacizumab has an estimated 60-day mortality of 25%.2 The diagnosis is confirmed by radiographs or CT of the abdomen demonstrating intraperitoneal free air, pneumatosis intestinalis, or portal venous gas. While management is generally surgical, supportive care, including antibiotics, parenteral nutrition, and fluid resuscitation, has been successful in poor surgical candidates.
In summary, we report a case of bowel perforation related to bevacizumab therapy. This case demonstrates the potentially life-threatening side effects of bevacizumab and other frequently-used, targeted therapies requiring ED diagnosis and resuscitation, and the complex imaging findings associated with the diagnosis of bowel perforation in a patient with recurrent ovarian cancer.
Footnotes
Section Editor: Rick A. McPheeters, DO
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
The documented Institutional Review Board Policy has been obtained and filed for publication of this case report.
Address for Correspondence: Samuel Burleson, MD, University of Alabama at Birmingham, Department of Emergency Medicine, Old Hillman Building Suite 251, 619 19th St. S, Birmingham, AL 35249. Email: slburleson@uabmc.edu. 4:227 – 229
Submission history: Revision received October 5, 2019; Submitted December 20, 2019; Accepted January 28, 2020
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Liu FW, Cripe J, Tewari KS. Anti-angiogenesis therapy in gynecologic malignancies. Oncology (Williston Park). 2015;29:350-60.
2. Badgwell BD, Camp ER, Feig B, et al. Management of bevacizumab-associated bowel perforation: a case series and review of the literature. Ann Oncol 2007. ;19:577-82.
3. Bamias A, Gibbs E, Khoon Lee C, et al. Bevacizumab with or after chemotheraphy for platinum-resistant recurrent ovarian cancer: exploratory analyses of the AURELIA trial. Ann Oncol. 2017;28:1842-8.
4. Han E, Monk B. What is the risk of bowel perforation associated with bevacizumab therapy in ovarian cancer?. Gynecol Oncol. 2007;105:3-6.
5. Burger RA, Brady MF, Bookman MA, et al. Risk factors for GI adverse events in a phase III randomized trial of bevacizumab in first-line therapy of advanced ovarian cancer: a gynecologic oncology group study. J Clin Oncol. 2014;32:1210-7.
6. Thornton E, Howard SA, Jagannathan J, et al. Imaging features of bowel toxicities in the setting of molecular targeted therapies in cancer patients. Br J Radiol. 2012;85(1018):1420-6.