
{kind=link}
| Author | Affiliation |
|---|---|
| Gary Lai, DO | Broward Health, Department of Emergency Medicine, Coral Springs, Florida |
| Brett Staller, MD | Broward Health, Department of Diagnostic Radiology, Coral Springs, Florida |
| Bhaskar Ganguly, MD | Broward Health, Department of Internal Medicine, Coral Springs, Florida |
| Quan Ta, BS | Florida Atlantic University, Boca Raton, Florida |
| Alexander J. Scumpia, DO, MSc | Broward Health, Department of Emergency Medicine, Coral Springs, Florida |
ABSTRACT
A 19-year-old Asian male presented to our emergency department with atraumatic right hip pain radiating to the right groin associated with pain on ambulation. Magnetic resonance imaging of the right hip with and without contrast revealed the diagnosis. Pigmented villonodular synovitis is a rare, monoarticular benign tumor originating from the synovium of the joint. The treatment is synovectomy of the pathological joint to prevent further disease progression.
CASE PRESENTATION
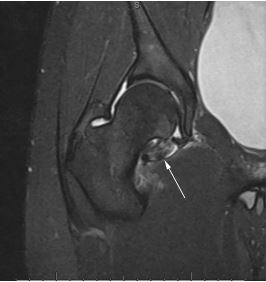
A 19-year-old Asian male presented to our emergency department (ED) with a one-day history of atraumatic right hip pain radiating to the right groin associated with pain on ambulation. The patient denied weakness or numbness of his extremity, fever, chills, or recent illness. Physical examination only revealed decreased range of motion and pain with internal rotation and flexion of the right hip. ED labs consisting of complete blood count, complete metabolic profile, C-reactive protein, and erythrocyte sedimentation rate were within normal limits. Ultrasound with Doppler of the patient’s scrotum was unremarkable. Computed tomography of the abdomen and pelvis with intravenous contrast demonstrated a right hip fluid collection consistent with inflammation or infection. Magnetic resonance imaging (MRI) of the right hip with and without contrast suggested the diagnosis (Image).
DISCUSSION
Pigmented villonodular synovitis
Pigmented villonodular synovitis (PVNS) is a rare, monoarticular benign tumor originating from the synovium of the joint.1,2 More commonly, this tumor is slow-growing, involving a localized portion of the joint or, in rarer cases, diffuse with malignant-type features (ie, involving the entire joint, or extra-articular lesions).3-5 The incidence of intra-articular PVNS predominately occurs in young adults (median age of 30 years) and has been reported to be 1.8 per million with equal gender distribution.4 The hip is the second most common joint affected (15% of all cases), with the knee the most prevalent of joints affected. MRI is the radiographic study of choice to identify hyperplastic synovium lesion(s) characteristic of PVNS.4 The treatment is complete synovectomy of the pathological joint to prevent further disease progression; with a recurrence rate of 7.7 to 17.8%.1 This case illustrates the necessity of a broad ED differential diagnosis (i.e., neoplasms, infection, etc.) accompanied with multiple diagnostic modalities for optimum patient outcome.
CPC-EM Capsule
What do we already know about this clinical entity?
Pigmented villonodular synovitis (PVNS) is a rare, monoarticular benign tumor originating from the synovium of the joint.
What is the major impact of the image(s)?
The image demonstrates the hypointense lesion caused by the hemosiderin deposition in the hyperplastic synovium characteristic of PVNS.
How might this improve emergency medicine practice?
This case illustrates the necessity of a broad differential diagnosis in a very common patient chief complaint (arthralgia) for optimum patient outcome.
Footnotes
Section Editor: Anna McFarlin, MD
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
Documented patient informed consent and/or Institutional Review Board approval has been obtained and filed for publication of this case report.
Address for Correspondence: Alexander J. Scumpia, DO, Broward Health, Department of Emergency Medicine, 3000 Coral Hills Dr, Coral Springs, FL 33065. Email: ascumpia@yahoo.com. 4:225 – 226
Submission history: Revision received September 16, 2019; Submitted December 6, 2019; Accepted December 19, 2019
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Steinmetz S, Rougemont AL, Peter R. Pigmented villonodular synovitis of the hip. EFFORT Open Rev. 2016;1(6):260-6.
2. Elumogo CO, Kochenderfer JN, Civelek AC, et al. Pigmented villonodular synovitis mimics metastases on fluorine 18 fluorodeoxyglucose position emission tomography-computed tomography. Quan Imaging Med Surg. 2016;6(2):218-23.
3. Koto K, Murata H, Sakabe T, et al. Magnetic resonance imaging and thallium-201 scintigraphy for the diagnosis of localized pigmented villonodular synovitis arising from the elbow: a case report and review of the literature. Exp Ther Med. 2013;5(5):1277-80.
4. Bertoni F, Unni KK, Beabout JW, et al. Malignant giant cell tumor of the tendon sheaths and joints (malignant pigmented villonodular synovitis). Am J Surg Pathol. 1997;21(2):153-63.
5. Shabat S, Kollender Y, Merimsky O, et al. The use of surgery and yttrium 90 in the management of extensive and diffuse pigmented villonodular synovitis of large joints. Rheumatology (Oxford). 2002;41(10):1113-8.