
{kind=link}
| Author | Affiliation |
|---|---|
| Adam J. Smith, MD | Maricopa Integrated Health System, Maricopa Medical Center, Emergency Medicine Residency, Phoenix, Arizona |
| Paul Blackburn, DO | Maricopa Integrated Health System, Maricopa Medical Center, Emergency Medicine Residency, Phoenix, Arizona |
CASE PRESENTATION
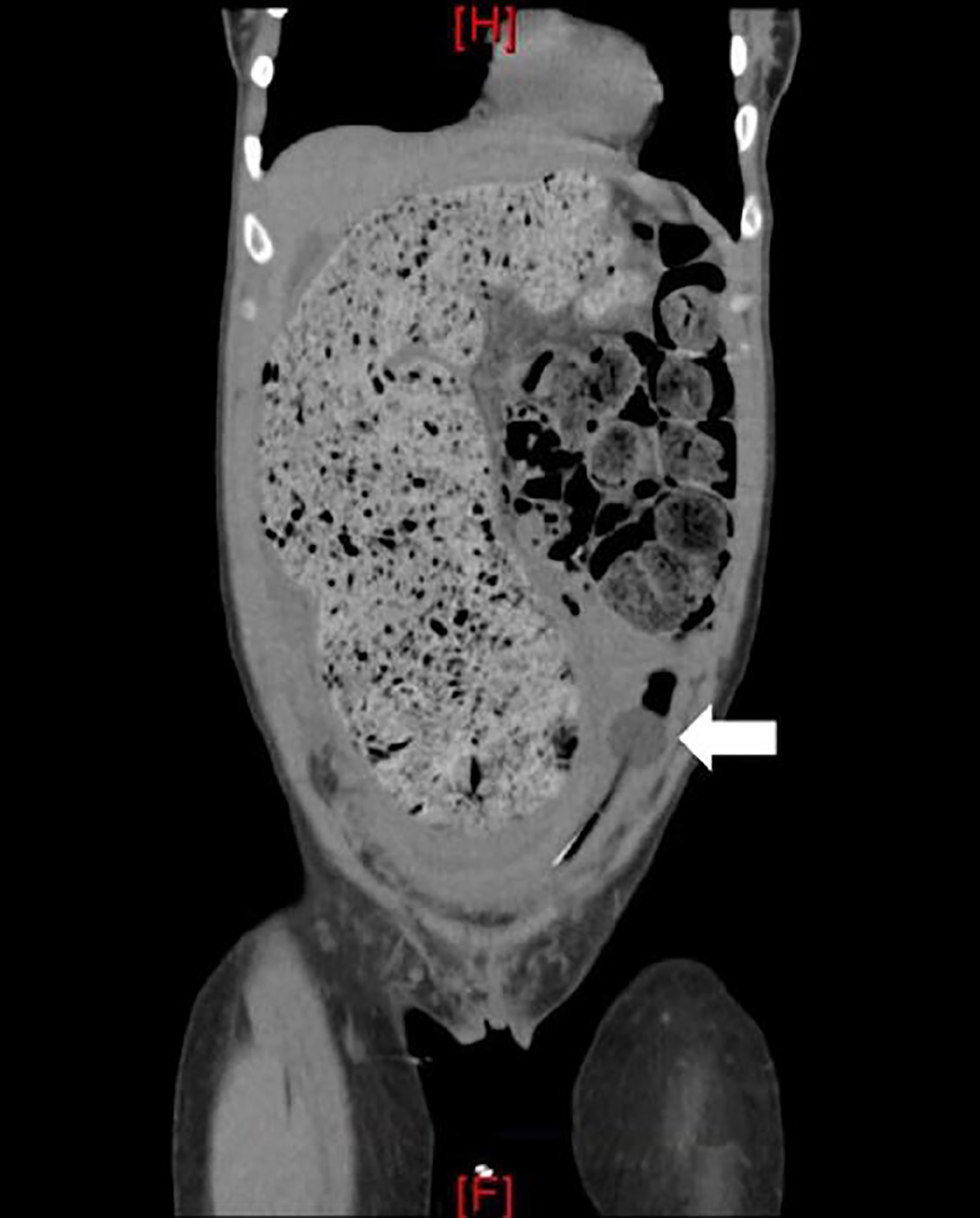
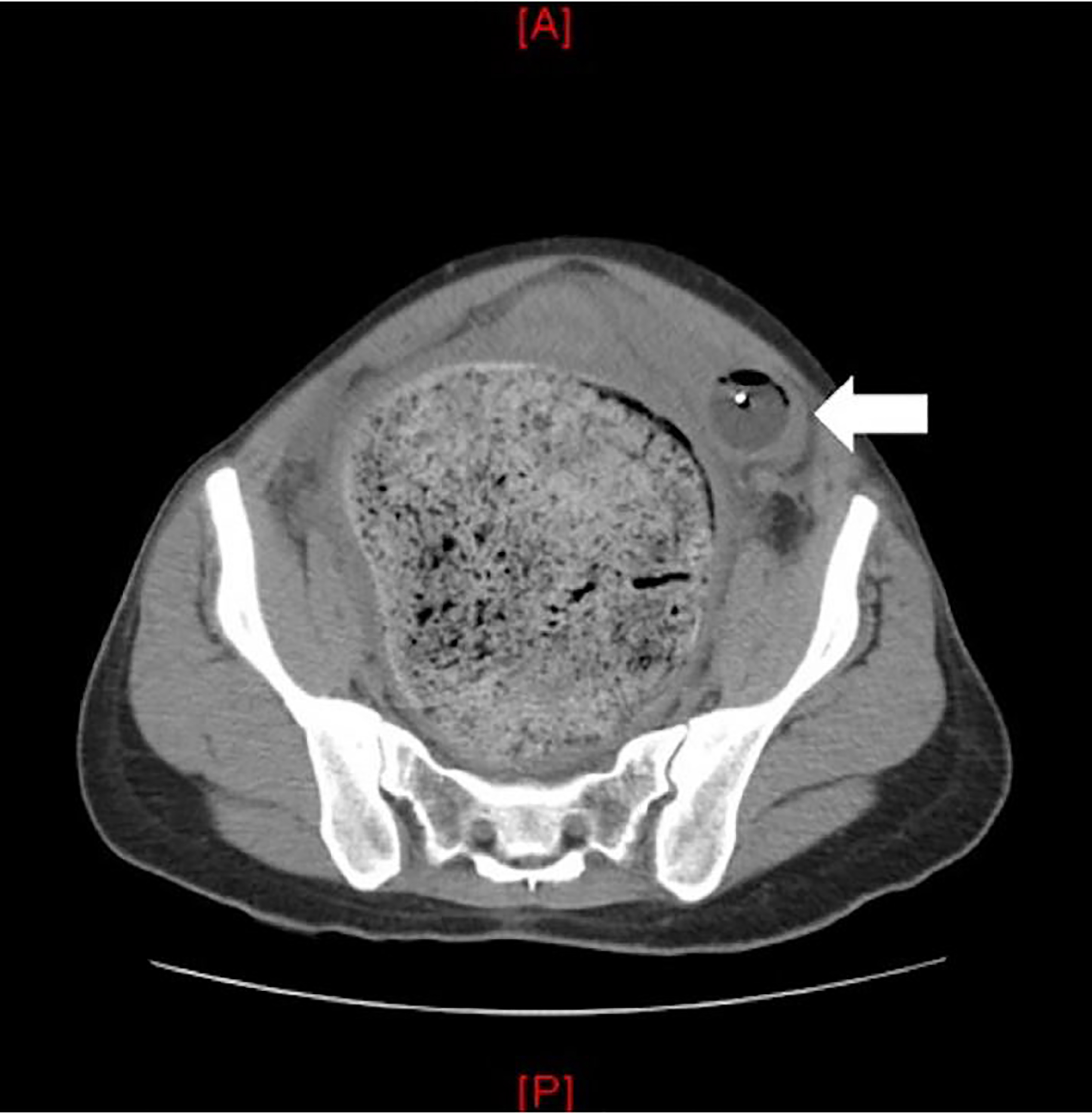
A 29-year-old female with a past medical history of constipation and anxiety, noted during previous pregnancies, presented with a chief complaint of acute urinary retention. She was not taking any medications and had no prior history of abdominal surgeries. She did report three previously uncomplicated pregnancies. Physical exam was significant for visible, firm suprapubic and right lower abdominal masses. Point-of-care ultrasonography demonstrated one liter of retained urine. An indwelling urinary catheter was inserted. The patient agreed to computed tomography (CT) for further evaluation (Images 1, 2, and 3).

DISCUSSION
Acute Urinary Retention Secondary to Chronic Constipation
CT imaging demonstrated severe idiopathic constipation causing megacolon and displacement of the bladder resulting in outlet obstruction. Acute urinary retention is uncommon in women with a prevalence of 1:100,000 women per year.1,2 Differential includes outflow obstruction, neurologic impairment, detrusor muscle weakness, medications (especially anticholinergics), and infection. Obstruction in women is generally secondary to anatomic distortion, including pelvic organ prolapse, pelvic masses, or urethral diverticulum.1,3
Constipation is an atypical cause of acute urinary retention in adults and is rarely mentioned in the literature.4 A sigmoid colon diameter of 6.5 cm at the pelvic brim is commonly used as a discriminating point for diagnosing megacolon.5 Treatment for severe chronic constipation and fecal impaction typically includes manual disimpaction and enemas, or oral solutions containing polyethylene glycol. Patients should receive Gastroenterology referral for colonic transit and motility studies. A patient may require partial colectomy if conservative medical therapy fails.6,7,8,9
CPC-EM Capsule
What do we already know about this clinical entity?
Acute urinary retention in women is most commonly secondary to anatomic distortion but may also be caused by medications, infection, and neurologic disease.
What is the major impact of the image(s)?
These images highlight the severity of the anatomic distortion that results from severe chronic constipation.
How might this improve emergency medicine practice?
Consider close follow up or admission for surgical and gastroenterology evaluation and to assess for other underlying causes and resolution of obstruction.
Documented patient informed consent and/or Institutional Review Board approval has been obtained and filed for publication of this case report.
Footnotes
Section Editor: Rick A. McPheeters, DO
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
Address for Correspondence: Adam J. Smith, MD, Maricopa Integrated Health System, Maricopa Medical Center, Department of Emergency Medicine, 2601 E Roosevelt St. Phoenix, AZ 85008. Email: Adam.Smith@MIHS.org. 2:171 – 172
Submission history: Revision received December 8, 2017; Submitted February 16, 2018; Accepted February 28, 2018
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Ramsey S, Palmer M. The management of female urinary retention. Int Urol Nephrol. 2006;38(3–4):533-5.
2. Klarskov P, Andersen JT, Asmussen CF, et al. Acute urinary retention in women: a prospective study of 18 consecutive cases. Scand J Urol Nephrol. 1987;21(1):29-31.
3. Selius BA, Subedi R. Urinary retention in adults: diagnosis and initial management. Am Fam Physician. 2008;77(5):643-50.
4. Traslaviña GA, Del Ciampo LA, Ferraz IS. Acute urinary retention in a pre-school girl with constipation. Rev Paul Pediatr. 2015;33(4):488-92.
5. Preston DM, Lennard-Jones JE, Thomas BM. Towards a radiologic definition of idiopathic megacolon. Gastrointest Radiol. 1985;10(2):167-9.
6. Dipalma JA, Cleveland MV, McGowan J, et al. A randomized, multicenter, placebo-controlled trial of polyethylene glycol laxative for chronic treatment of chronic constipation. Am J Gastroenterol. 2007;102(7):1436-41.
7. Brandt LJ, Boley SJ. AGA technical review on intestinal ischemia. Gastroenterology. 2000;118(5):954-68.
8. Hernu R, Cour M, Wallet F, Argaud L. Threatening fecal impaction. J Emerg Med. 2017;52(1):13-5.
9. Khawaja MR, Akhavan N, Chiorean M. Chronic constipation with megacolon. J Gen Intern Med. 2011;26(8):938.