
{kind=link}
| Author | Affiliation |
|---|---|
| Jonathan Rowland, MD | Wayne State University School of Medicine, Department of Emergency Medicine, Detroit, Michigan |
| Lauren Traill, MD | Wayne State University School of Medicine, Department of Emergency Medicine, Detroit, Michigan |
| Mark Favot, MD | Wayne State University School of Medicine, Department of Emergency Medicine, Detroit, Michigan |
CASE PRESENTATION
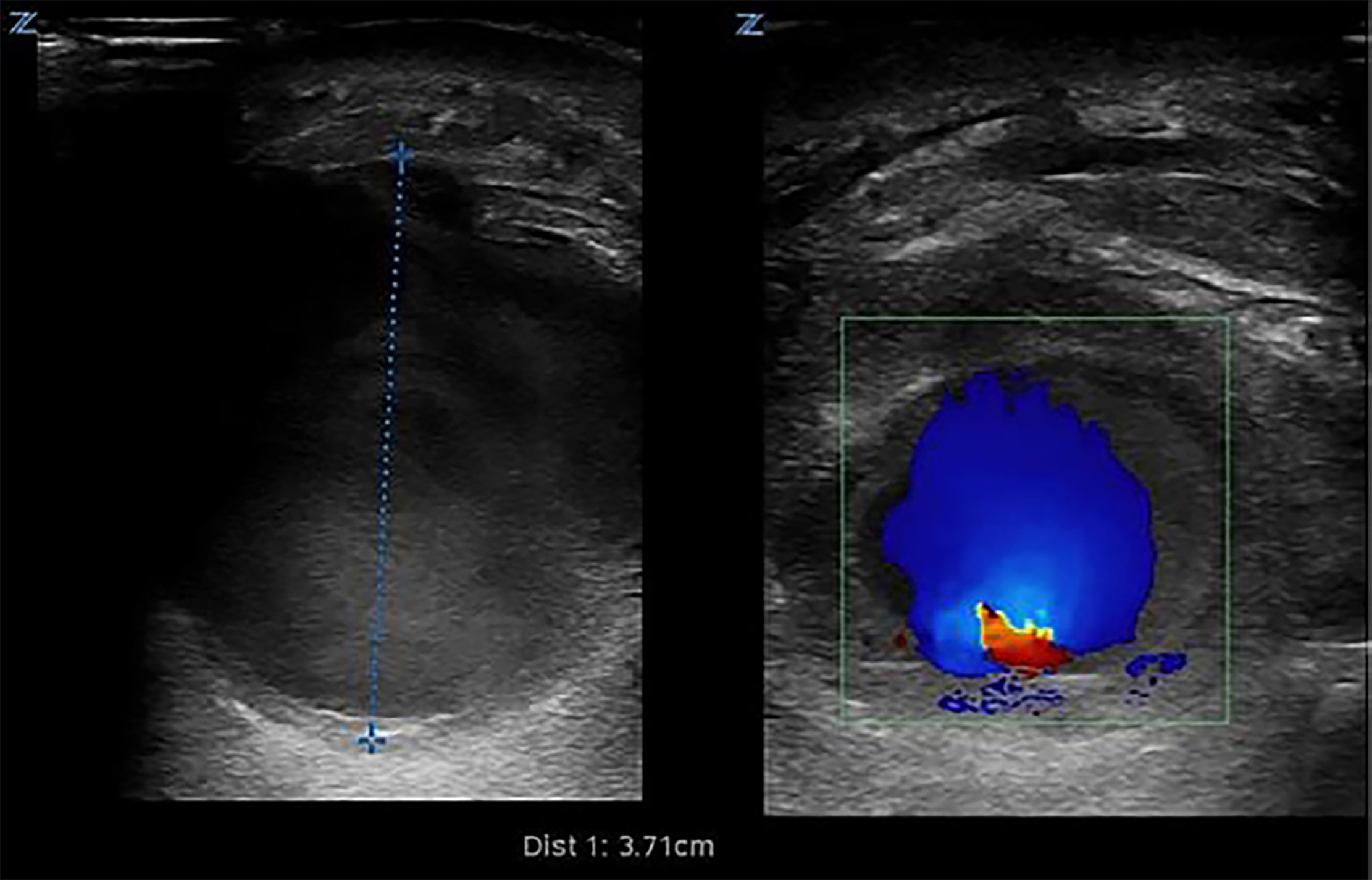
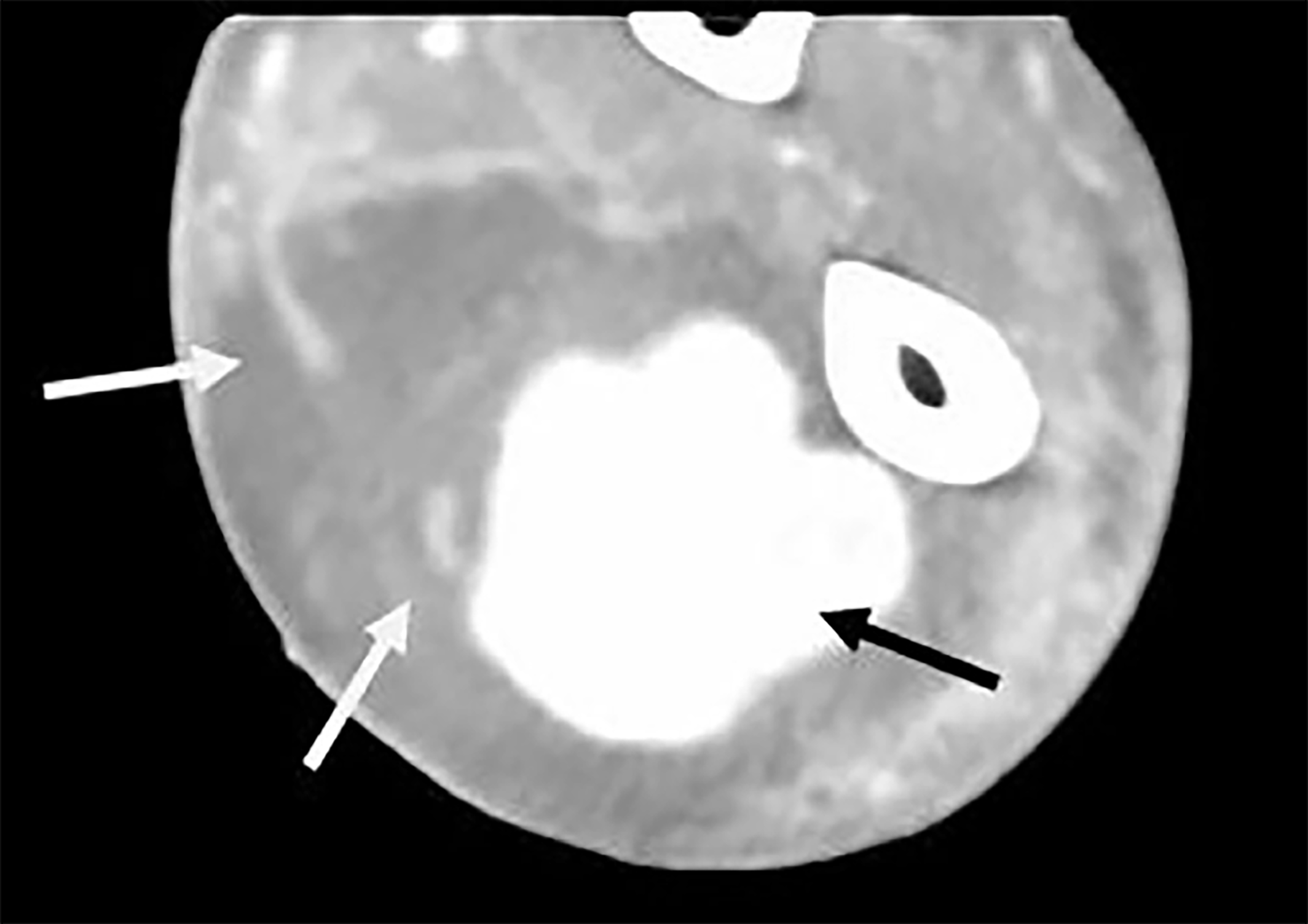
A 64-year-old male with a history of intravenous drug abuse presented to the emergency department (ED) with left arm pain and swelling for four days. Left upper extremity exam revealed diffuse swelling, erythema and tenderness in the mid-distal forearm. A point-of-care ultrasound (POCUS) was performed to characterize the suspected abscess for incision and drainage; however, imaging revealed a severely enlarged radial artery, suspected to be a pseudoaneurysm with an approximate diameter of 3.71 cm (Image 1, Video). Computed tomography of the extremity revealed an aneurysmal radial artery (Image 2). The patient was transferred to the operating room where the diagnosis was revealed.
DIAGNOSIS
Radial Artery Mycotic Aneurysm
Mycotic aneurysms are rare, with annual prevalence of 0.03% of injection drug users who present to the ED with complications from injection.1 Far more common is the development of an abscess or cellulitis at the injection site. However, due to the lethality of attempted blind incision and drainage of an aneurysm or pseudoaneurysm, it is critical to properly distinguish these from an abscess or cellulitis.
POCUS is a safe, accurate, and cost-effective modality to distinguish between these diagnoses, and can alter management by 73% when compared to clinical judgment.2 The sonographic appearances of an abscess and cellulitis have been well described.3 An abscess most commonly has an anechoic or hyperechoic spherical appearance with lobulated or irregular borders as well as possible posterior acoustic enhancement.4,5 The use of color Doppler to identify any blood flow within an anechoic structure can be a critical step to avoid a catastrophic incision into a blood-filled structure. The patient was taken to the operating room where surgeons revealed a purulent aneurysmal radial artery that was treated with ligation and debridement, parenteral antibiotics, and wound vacuum dressings.
CPC-EM Capsule
What do we already know about this clinical entity?
Mycotic aneurysm is a rare but serious presentation among intravenous drug abusers presenting with seemingly classic skin and soft tissue infection at injection sites.
What is the major impact of the image(s)?
Point-of-care ultrasound (POCUS) of suspected abscesses prior to incision and drainage is an effective method of securing this diagnosis and ensuring you are not incising something else.
How might this improve emergency medicine practice?
This case further supports the use of POCUS in helping emergency providers to avoid rare but potentially catastrophic complications during routine abscess evaluation and management.
Documented patient informed consent and/or Institutional Review Board approval has been obtained and filed for publication of this case report.
Footnotes
Section Editor: Rick A. McPheeters, DO
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
Address for Correspondence: Mark Favot, MD, Wayne State University School of Medicine, Department of Emergency Medicine, 6071 W. Outer Dr. Lourdes 447-D, Detroit, MI 48235. Email: mfavot@med.wayne.edu. 2:371 – 372
Submission history: Revision received May 27, 2018; Submitted July 16, 2018; Accepted July 18, 2018
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Tsao JW, Marder SR, Goldstone J, et al. Presentation, diagnosis, and management of arterial mycotic pseudoaneurysms in injection drug users. Ann Vasc Surg. 2002;16(5):652-62.
2. Adhikari S, Blaivas M. Sonography first for subcutaneous abscess and cellulitis evaluation. J Ultrasound Med. 2012;31(10):1509-12.
3. Subramaniam S, Bober J, Chao J, et al. Point-of-care ultrasound for diagnosis of abscess in skin and soft tissue infections. Acad Emerg Med. 2016;23(11):1298-306.
4. Gaspari RJ, Blehar D, Polan D, et al. The Massachusetts Abscess Rule: a clinical decision rule using ultrasound to identify methicillin-resistant in skin abscesses. Acad Emerg Med. 2014;21(5):558-67.
5. Nelson CE, Chen AE, Bellah RD, et al. Ultrasound features of purulent skin and soft tissue infection without abscess. Emerg Radiol. 2018.
SUPPLEMENTARY MATERIAL
Radial artery mycotic aneurysm.