
{kind=link}
| Author | Affiliation |
|---|---|
| Alexander W. Hirsch, MD | Boston Children’s Hospital, Harvard Medical School, Division of Emergency Medicine, Boston, Massachusetts |
| Erica Y. Popovsky, MD | Boston Children’s Hospital, Harvard Medical School, Division of Emergency Medicine, Boston, Massachusetts |
| Lise E. Nigrovic, MD, MPH | Boston Children’s Hospital, Harvard Medical School, Division of Emergency Medicine, Boston, Massachusetts |
| Michele M. Burns, MD | Boston Children’s Hospital, Harvard Medical School, Division of Emergency Medicine, Boston, Massachusetts |
CASE PRESENTATION
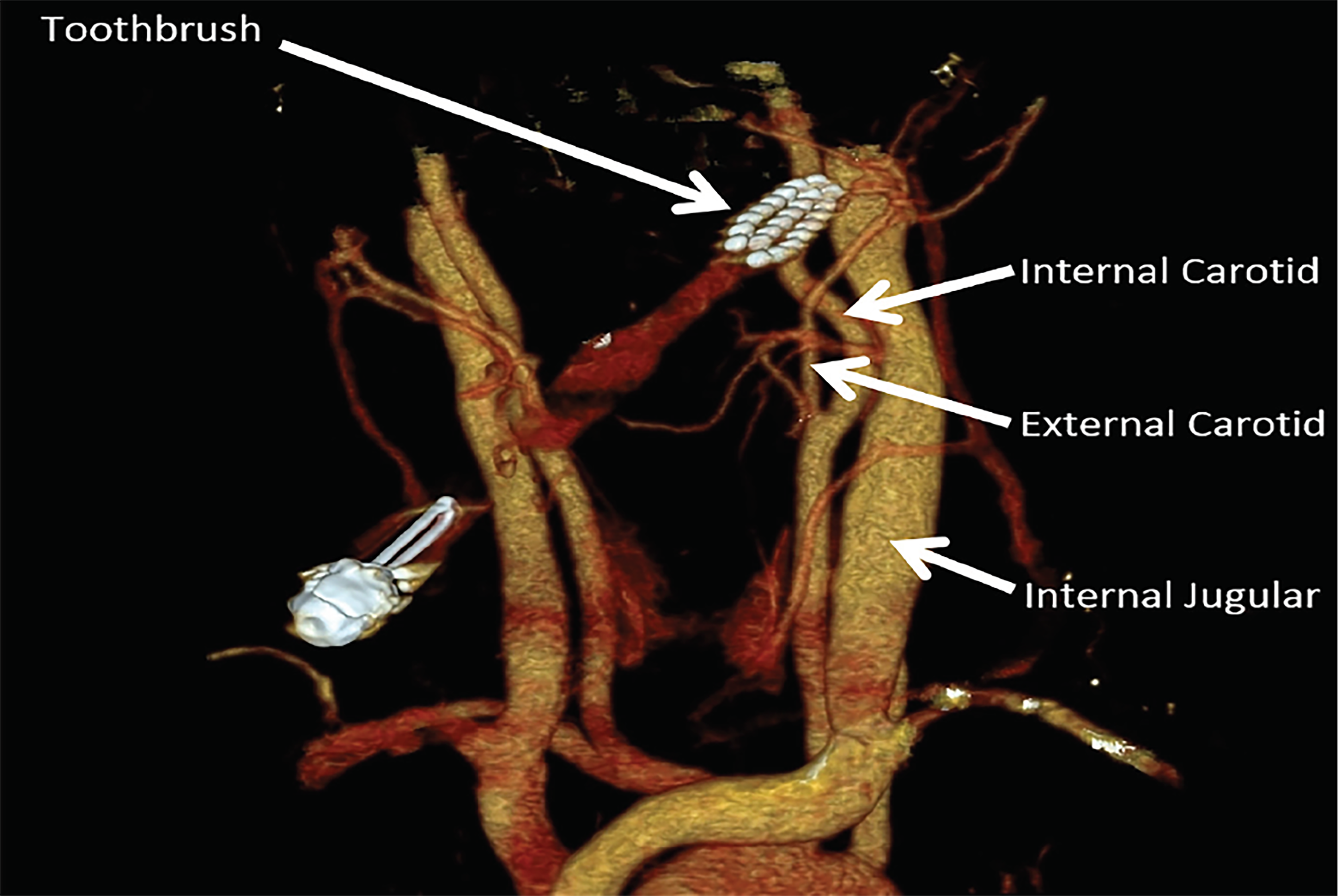
A five-year-old male presented to the emergency department (ED) after falling off a stool while brushing his teeth, resulting in a penetrating oropharyngeal injury. The toothbrush was impaled deeply into the left lateral soft palate with only the handle of the toothbrush visible protruding from the mouth. The patient was hemodynamically stable and was comfortable in the arms of his mother after a single dose of fentanyl. A computed tomography angiography (CTA) with three-dimensional reconstructions was performed without sedation, which showed the tip of the toothbrush terminating adjacent to the alveolar and pterygoid branches of the external carotid artery, but with no visible injury to these vessels (Image). Associated subcutaneous emphysema and muscle edema were also noted. The otorhinolaryngology service was consulted, and the toothbrush was successfully removed in the operating room without complication.
DISCUSSION
Although the distance from the tonsillar fossa to the internal carotid artery is approximately only 25 millimeters,1 most children with penetrating oropharyngeal trauma can be managed expectantly. Rarely, these injuries can damage the internal carotid artery leading to thrombosis or dissection of the affected vessel risking a cerebrovascular accident.2,3 In a previous single-center cohort of children with penetrating palate trauma, the risk of stroke was 0% (95% confidence interval 0–2.5%).4 Although most patients with penetrating palate injuries do not require imaging, CTA is the first-line imaging modality for the ED clinicians with a sensitivity between 90–100% for vascular injury when compared to angiography.5
CPC-EM Capsule
What do we already know about this clinical entity?
Children with penetrating oropharyngeal trauma are at risk for vascular injury, although vascular complications are rare.
What is the major impact of the image(s)?
The image demonstrates the proximity of the vasculature to the soft palate and highlights the potential for vascular injury.
How might this improve emergency medicine practice?
Most penetrating oropharyngeal injuries do not require imaging, but if the exam or mechanism is concerning, computed tomography angiography should be the first-line imaging modality.
Documented patient informed consent and/or Institutional Review Board approval has been obtained and filed for publication of this case report.
Footnotes
Section Editor: Rick A. McPheeters, DO
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
Address for Correspondence: Alexander W Hirsch, MD, Boston Children’s Hospital, Division of Emergency Medicine, 300 Longwood Ave, Boston, MA 02115. Email: alexander.hirsch@childrens.harvard.edu. 2:373 – 374
Submission history: Revision received May 28, 2018; Submitted August 4, 2018; Accepted August 8, 2018
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Deutsch MD, Kriss VM, Willging JP. Distance between the tonsillar fossa and internal carotid artery in children. Arch Otolaryngol Head Neck Surg. 1995;121(12):1410-2.
2. Zonfrillo MR, Roy AD, Walsh SA. Management of pediatric penetrating oropharyngeal trauma. Pediatr Emerg Care. 2008;24(3):172-5.
3. Melio FR, Jones JL, Djang WT. Internal carotid artery thrombosis in a child secondary to intraoral trauma. J Emerg Med. 1996;14(4):429-33.
4. Hennelly K, Kimia A, Lee L, et al. Incidence of morbidity from penetrating palate trauma. Pediatrics. 2010;126(6):e1578-84.
5. Brietzke SE, Jones DT. Pediatric oropharyngeal trauma: what is the role of CT scan?. Int J Pediatr Otorhinolaryngol. 2005;69(5):669-79.