
{kind=link}
| Author | Affiliation |
|---|---|
| Gregory Mansella, MD | University Hospital Basel, Department of Emergency Medicine, Basel, Switzerland |
| Raban Jeger, MD | University Hospital Basel, Department of Cardiology, Basel, Switzerland |
| Roland Bingisser, MD | University Hospital Basel, Department of Emergency Medicine, Basel, Switzerland |
| Christian H. Nickel, MD | University Hospital Basel, Department of Emergency Medicine, Basel, Switzerland |
Introduction
Case report
Discussion
Conclusion
ABSTRACT
A 36-year-old man was brought to our emergency department after successful resuscitation of out-of-hospital cardiac arrest with the whole spectrum of neurocardiogenic effects in subarachnoid hemorrhage: electrocardiographic changes, regional wall motion abnormalities, and elevations of cardiac enzymes. Coronary angiography revealed normal coronary arteries but showed the midventricular type of Takotsubo cardiomyopathy in the left ventriculography. Subsequently, cerebral computed tomography revealed diffuse subarachnoid hemorrhage and generalized cerebral edema with brain herniation. Brain death was diagnosed. This case highlights the possibility of an acute cerebral illness (especially subarachnoid hemorrhage) as an underlying cause of cardiac abnormalities mimicking myocardial ischemia.
INTRODUCTION
Subarachnoid hemorrhage accounts for 10% of hemorrhagic strokes, most of which are caused by ruptured saccular aneurysms with a mortality rate of up to 50%.1 Most deaths occur within the first two days of onset, with the majority related to the initial hemorrhage.2 Complications resulting from subarachnoid hemorrhage are rebleeding,3 vasospasm and delayed cerebral ischemia,4 hydrocephalus,5 increased intracranial pressure,6 seizures7 and hyponatremia.8 Cardiac abnormalities such as electrocardiographic changes, left ventricular dysfunction, and troponin elevations mimicking myocardial ischemia can also occur.
CASE REPORT
A 36-year-old man was brought to our emergency department (ED) by emergency medical services after witnessed loss of consciousness in a public toilet. No medical history regarding symptoms before collapse, significant health issues, or illicit or recreational drug use was known at ED arrival. When the paramedics arrived at the scene, the patient was in asystole. After 10 minutes of cardiopulmonary resuscitation the patient showed return of spontaneous circulation (ROSC) and was transported to our ED after intubation on scene.
In the ED, blood pressure was 85/40 mmHg, heart rate 120 bpm and oxygen saturation was 98% on mechanical ventilation (FiO2 100%). Heart sounds were regular with no murmurs and the lungs were clear to auscultation bilaterally. Glasgow Coma Scale was 3, pupils were dilated with minimal pupillary response and Babinski’s reflex was negative bilaterally.
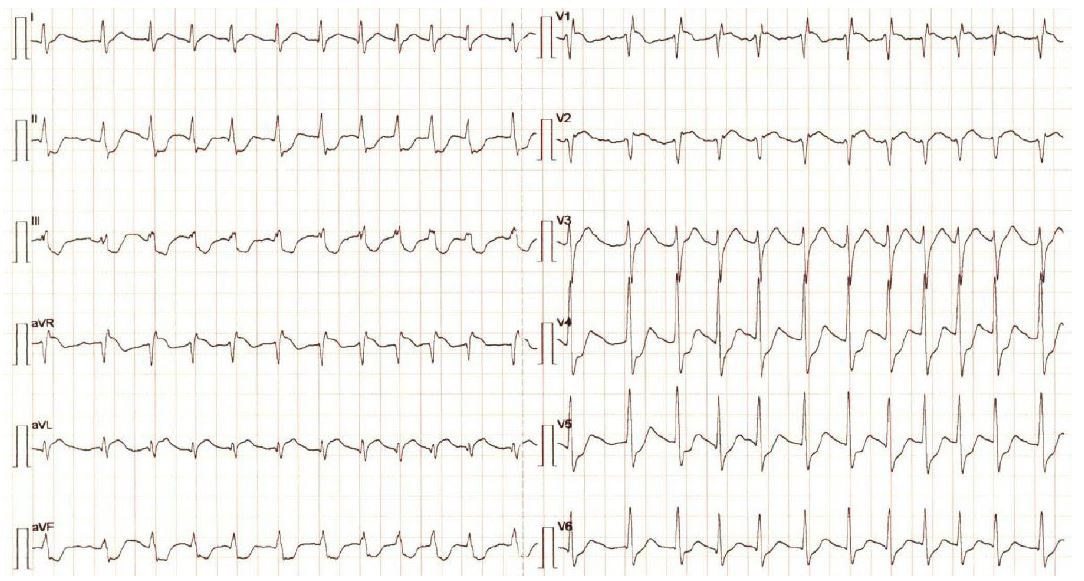
The electrocardiogram showed a narrow complex tachycardia with 150 bpm, ST-segment elevation in leads aVR, V1, V2 and ST-segment depression in leads II, III, aVF and V4 to V6 (Image 1).
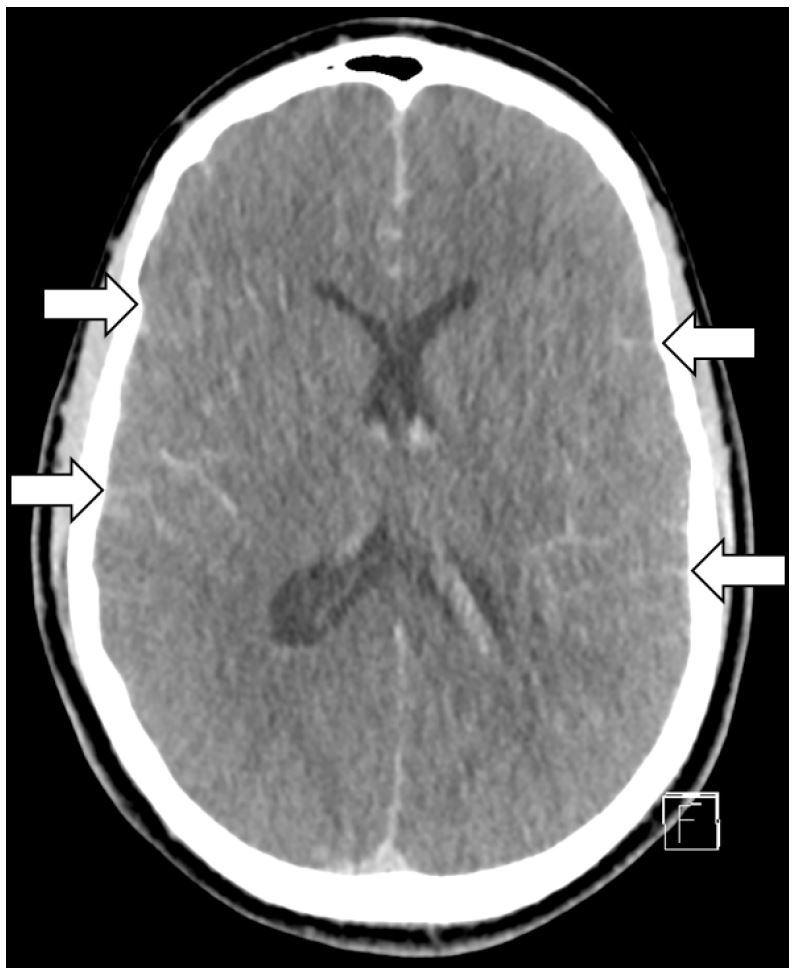
Laboratory exams showed increased levels of high sensitive cardiac troponin T, creatine kinase and brain type natriuretic peptide. Suspecting fatal arrhythmia due to myocardial infarction as underlying cause, the patient was treated with aspirin and low molecular weight heparin. Acute coronary angiography was performed, which revealed normal coronary arteries, but demonstrated the midventricular type of Takotsubo cardiomyopathy in the left ventriculography. The left ventricular function was impaired with an ejection fraction of 47%. For further diagnostic workup, cerebral computed tomography with angiography was performed showing diffuse subarachnoid hemorrhage extending into the ventricular system due to a ruptured basilar artery aneurysm, and generalized cerebral edema with brain herniation and absent peripheral perfusion (Image 2).
According to his clinical presentation with persistent Glasgow Coma Scale of 3 without analgosedation and decerebrate posturing (adducted and extended arms with pronated wrists and flexed fingers, as well as extended legs with plantar flexion of the feet), the Hunt and Hess score was 5 (Table 1).
| Grade | Neurologic status |
|---|---|
| 1 | Asymptomatic, or minimal headache and slight nuchal rigidity |
| 2 | Moderate to severe headache, nuchal rigidity, no neurologic deficit other than cranial nerve palsy |
| 3 | Drowsiness, confusion, or mild focal neurologic deficit |
| 4 | Stupor, moderate or severe hemiparesis, possibly early decerebrate rigidity and vegetative disturbances |
| 5 | Deep coma, decerebrate rigidity, moribund appearance |
Because of persistent shock the patient was treated in the ED with epinephrine infusion with a maximum dose up to 0.3 mcg/kg/minute. Due to severe subarachnoid hemorrhage and loss of brainstem reflexes no additional intervention was recommended by neurosurgery. For further care the patient was transferred to our intensive care unit. Brain death was diagnosed by a neurologist and an intensive care physician who performed an apnea test. The family denied consent to organ donation.
DISCUSSION
It is speculated that cardiac dysfunction after subarachnoid hemorrhage is most likely caused by centrally mediated release of catecholamines within the myocardium due to hypoperfusion of the posterior hypothalamus.10-12 Histological analysis of myocardial tissue in patients after subarachnoid hemorrhage typically demonstrated subendocardial contraction band necrosis, also known as myocytolysis, without coagulation necrosis, as found in myocardial infarction.13-20 Clinically, the neurocardiogenic effects of subarachnoid hemorrhage may present with electrocardiographic changes, elevations of troponin and/or brain type natriuretic peptide, as well as regional wall motion abnormalities, including Takotsubo cardiomyopathy.
Depending on the study, electrocardiographic abnormalities occur in 27% up to 100% of patients with subarachnoid hemorrhage.21-25 The most striking electrocardiographic abnormalities are found within the first 48 to 72 hours,21-22 which are summarized in Table 2.
| Morphological changes | Rhythm disturbances |
|---|---|
| peaked P-wave, short PR-interval | sinus bradycardia, sinus tachycardia |
| high R-wave | wandering atrial pacemaker, atrial fibrillation, atrial flutter |
| ST-segment elevation, ST-segment depression | atrioventricular block |
| QT-interval prolongation | premature atrial, junctional, ventricular complexes |
| deep symmetric T-wave inversion | ventricular tachycardia (including Torsades de Pointes) |
| prominent U-wave |
ST-segment elevation typically is found in the precordial leads34 and seems to occur mainly in those with apical and midventricular regional wall motion abnormalities.35-36 QT-interval prolongation is more common with subarachnoid hemorrhage than with other forms of acute cerebrovascular disease and is responsible for the greater relative risk of ventricular tachyarrhythmia.37-39 Therefore, constant electrocardiographic monitoring in the acute phase of subarachnoid haemorrhage is recommended.
The electrocardiographic changes are predominantly reflective of ischemic changes in the subendocardium of the left ventricle due to the release of large amounts of catecholamines. The diagnosis of myocardial injury in subarachnoid hemorrhage can be established by elevation of serum troponin, which can be observed in approximately 20% to 40% of patients, depending on the used troponin assay.11,18,40-42 The elevation of troponin is usually mild to moderate and less pronounced than in myocardial infarction.42
Elevated peak troponin levels are associated with an increased mortality and worse functional outcome.43 Elevated brain type natriuretic peptide levels can be detected after subarachnoid haemorrhage as well,44-46 probably due to hypoxia of the hypothalamus, endothelin-1 release, and excess catecholamine secretion, which increases the after load on the cardiac ventricles.47,48 Elevated brain type natriuretic peptide levels have been associated with impaired left ventricular function,49 cerebral vasospasm and delayed ischemic neurological deficits,50 as well as increased mortality.51
Acute left ventricular systolic dysfunction is a well-recognized complication after subarachnoid haemorrhage,20,52-56 occurring in up to 30% of patients. This has been referred to as neurogenic stress cardiomyopathy or neurogenic stunned myocardium.20 Left ventricular systolic dysfunction usually develops within the first two days after subarachnoid hemorrhage. The timing of recovery of left ventricular systolic dysfunction ranges from a few days to weeks.53,56-61 Independent predictors of neurogenic stunned myocardium after subarachnoid hemorrhage include severity of neurological injury, troponin, creatine kinase-MB and brain type natriuretic peptide elevation as well as female gender.11,20,52 Patients with neurogenic stunned myocardium are at particularly high risk for potentially fatal complications such as ventricular arrhythmias.33 Furthermore, neurogenic stunned myocardium is associated with an increased risk of subarachnoid hemorrhage-associated cerebral vasospasm. It is likely that the alteration in cerebral perfusion associated with subarachnoid hemorrhage, combined with impaired left ventricular systolic dysfunction, contributes to vasospasm severity.62
The most common wall motion abnormalities in neurogenic stunned myocardium due to subarachnoid hemorrhage appear to be either global hypokinesis or the basal and midventricular type of Takotsubo cardiomyopathy. The classical apical type Takotsubo cardiomyopathy is less common.35,36,53,54,56,63 The exact reason for the different regional wall motion abnormalities in neurogenic stunned myocardium is not known. It might be explained by the unequal distribution of adrenergic receptors in myocardial cells, adrenergic receptor polymorphisms, and variations in individual susceptibilities to the circulating catecholamines in certain regions of the heart. Areas with higher density of adrenergic receptors may determine the area of hypokinesis.64-66
In our patient, neurogenic stress cardiomyopathy was difficult to distinguish from acute myocardial infarction given the associated electrocardiogram changes. Potential indicators that favor a diagnosis of neurogenic stunned myocardium include wall motion abnormalities disconcordant with a single epicardial coronary distribution and a relatively minor cardiac troponin release relative to the magnitude of left ventricular dysfunction.41 Despite these features, coronary angiography may be required in the acute setting to distinguish between neurogenic stunned myocardium and acute myocardial infarction in some patients, especially those after cardiac arrest as our patient.
Clinical management of patients with neurogenic stunned myocardium is generally supportive because left ventricular function usually normalizes spontaneously within a few days to weeks.53,56-61 It is important to exclude dynamic left ventricular outflow tract obstruction with echocardiography in patients with severe heart failure or significant hypotension.67,68 Whenever possible, the precipitating cause of neurogenic stunned myocardium should be addressed. In the absence of contraindications, β-blockers should be considered early to temper the catecholamine surge, and angiotensin converting enzyme inhibitors should be given until left ventricular function completely recovers. Diuretics are effective in most cases of congestive heart failure. Patients with cardiogenic shock should be treated with standard therapies including inotropes (in the absence of dynamic left ventricular outflow tract obstruction) and mechanical ventilation as needed.69
CONCLUSION
This case highlights the potential severity of the cardiac manifestations of subarachnoid hemorrhage as well as the need to consider a cerebral illness (especially subarachnoid hemorrhage) as a cause of electrocardiographic changes suggestive of myocardial infarction, troponin elevations and regional wall motion abnormalities, in order to avoid possible inappropriate or delayed therapy. In cases with absent clinical context of acute coronary syndrome, or a history of thunderclap headache, potentially harmful antiplatelet and anticoagulation therapies should be delayed until coronary artery disease involvement has been proven.
Footnotes
Section Editor: Rick A. McPheeters, DO
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
Address for Correspondence: Gregory Mansella, MD, University Hospital Basel, Department of Emergency Medicine, Petersgraben 2, 4031 Basel, Switzerland. Email: gregory.mansella@usb.ch. 1:16 – 21
Submission history: Revision received September 18, 2016; Submitted October 19, 2016; Accepted November 4, 2016
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Hop JW, Rinkel GJ, Algra A, et al. Case-fatality rates and functional outcome after subarachnoid hemorrhage: a systematic review. Stroke. 1997;28(3):660-4.
2. Broderick JP, Brott TG, Duldner JE, et al. Initial and recurrent bleeding are the major causes of death following subarachnoid hemorrhage. Stroke. 1994;25(7):1342-7.
3. Larsen CC, Astrup J. Rebleeding after aneurysmal subarachnoid hemorrhage: a literature review. World Neurosurg. 2013;79(2):307-12.
4. de Rooij NK, Rinkel GJ, Dankbaar JW, et al. Delayed cerebral ischemia after subarachnoid hemorrhage: a systematic review of clinical, laboratory, and radiological predictors. Stroke. 2013;44(1):43-54.
5. Sheehan JP, Polin RS, Sheehan JM, et al. Factors associated with hydrocephalus after aneurysmal subarachnoid hemorrhage. Neurosurgery. 1999;45(5):1120-7.
6. Heuer GG, Smith MJ, Elliott JP, et al. Relationship between intracranial pressure and other clinical variables in patients with aneurysmal subarachnoid hemorrhage. J Neurosurg. 2004;101(3):408-16.
7. Claassen J, Peery S, Kreiter KT, et al. Predictors and clinical impact of epilepsy after subarachnoid hemorrhage. Neurology. 2003;60(2):208-14.
8. Sherlock M, O’Sullivan E, Agha A, et al. The incidence and pathophysiology of hyponatraemia after subarachnoid haemorrhage. Clin Endocrinol (Oxf). 2006;64(3):250-4.
9. Hunt WE, Hess RM. Surgical risk as related to time of intervention in the repair of intracranial aneurysms. J Neurosurg. 1968;28(1):14-20.
10. Sakr YL, Ghosn I, Vincent JL. Cardiac manifestations after subarachnoid hemorrhage: a systematic review of the literature. Prog Cardiovasc Dis. 2002;45(1):67-80.
11. Tung P, Kopelnik A, Banki N, et al. Predictors of neurocardiogenic injury after subarachnoid hemorrhage. Stroke. 2004;35(2):548-51.
12. Lyon AR, Rees PS, Prasad S, et al. Stress (Takotsubo) cardiomyopathy–a novel pathophysiological hypothesis to explain catecholamine-induced acute myocardial stunning. Nat Clin Pract Cardiovasc Med. 2008;5(1):22-9.
13. Sugiura M, Yozawa Y, Kubo O, et al. Myocardial damage (myocytolysis) caused by subarachnoid hemorrhage. No To Shinkei. 1985;37(12):1155-61.
14. Karch SB, Billingham ME. Myocardial contraction bands revisited. Hum Pathol. 1986;17(1):9-13.
15. Samuels MA. Neurogenic heart disease: a unifying hypothesis. Am J Cardiol. 1987;60(18):15J-19J.
16. Elrifai AM, Bailes JE, Shih SR, et al. Characterization of the cardiac effects of acute subarachnoid hemorrhage in dogs. Stroke. 1996;27(4):737-41.
17. Zaroff JG, Rordorf GA, Titus JS, et al. Regional myocardial perfusion after experimental subarachnoid hemorrhage. Stroke. 2000;31(5):1136-43.
18. Parekh N, Venkatesh B, Cross D, et al. Cardiac troponin I predicts myocardial dysfunction in aneurysmal subarachnoid hemorrhage. J Am Coll Cardiol. 2000;36(4):1328-35.
19. Wittstein IS, Thiemann DR, Lima JA, et al. Neurohumoral features of myocardial stunning due to sudden emotional stress. N Engl J Med. 2005;352(6):539-48.
20. Lee VH, Oh JK, Mulvagh SL, et al. Mechanisms in neurogenic stress cardiomyopathy after aneurysmal subarachnoid hemorrhage. Neurocrit Care. 2006;5(3):243-9.
21. Di Pasquale G, Pinelli G, Andreoli A, et al. Holter detection of cardiac arrhythmias in intracranial subarachnoid hemorrhage. Am J Cardiol. 1987;59(6):596-600.
22. Brouwers PJ, Wijdicks EF, Hasan D, et al. Serial electrocardiographic recording in aneurysmal subarachnoid hemorrhage. Stroke. 1989;20(9):1162-7.
23. Solenski NJ, Haley EC, Kassell NF, et al. Medical complications of aneurysmal subarachnoid hemorrhage: a report of the multicenter, cooperative aneurysm study. Participants of the Multicenter Cooperative Aneurysm Study. Crit Care Med. 1995;23(6):1007-17.
24. Zaroff JG, Rordorf GA, Newell JB, et al. Cardiac outcome in patients with subarachnoid hemorrhage and electrocardiographic abnormalities. Neurosurgery. 1999;44(1):34-9.
25. Sommargren CE. Electrocardiographic abnormalities in patients with subarachnoid hemorrhage. Am J Crit Care. 2002;11(1):48-56.
26. Rudehill A, Olsson GL, Sundqvist K, et al. ECG abnormalities in patients with subarachnoid haemorrhage and intracranial tumours. J Neurol Neurosurg Psychiatry. 1987;50(10):1375-81.
27. Huang CC, Huang CH, Kuo HY, et al. The 12-lead electrocardiogram in patients with subarachnoid hemorrhage: early risk prognostication. Am J Emerg Med. 2012;30(5):732-6.
28. Junttila E, Vaara M, Koskenkari J, et al. Repolarization abnormalities in patients with subarachnoid and intracerebral hemorrhage: predisposing factors and association with outcome. Anesth Analg. 2013;116(1):190-7.
29. De Sweit J. Changes simulating hypothermia in the electrocardiogram in subarachnoid hemorrhage. J Electrocardiol. 1972;5(2):93-5.
30. Syverud G. Electrocardiographic changes and intracranial pathology. Aana J. 1991;59(3):229-32.
31. Eisalo A, Perasalo J, Halonen PI. Electrocardiographic abnormalities and some laboratory findings in patients with subarachnoid haemorrhage. Br Heart J. 1972;34(3):217-26.
32. Cruickshank JM, Neil-Dwyer G, Stott AW. Possible role of catecholamines, corticosteroids, and potassium in production of electrocardiographic abnormalities associated with subarachnoid haemorrhage. Br Heart J. 1974;36(7):697-706.
33. Estanol Vidal B, Badui Dergal E, Cesarman E, et al. Cardiac arrhythmias associated with subarachnoid hemorrhage: prospective study. Neurosurgery. 1979;5(6):675-80.
34. Sharkey SW, Windenburg DC, Lesser JR, et al. Natural history and expansive clinical profile of stress (tako-tsubo) cardiomyopathy. J Am Coll Cardiol. 2010;55(4):333-41.
35. Kono T, Morita H, Kuroiwa T, et al. Left ventricular wall motion abnormalities in patients with subarachnoid hemorrhage: neurogenic stunned myocardium. J Am Coll Cardiol. 1994;24(3):636-40.
36. Kuroiwa T, Morita H, Tanabe H, et al. Significance of ST segment elevation in electrocardiograms in patients with ruptured cerebral aneurysms. Acta Neurochir. 1995;133(3–4):141-6.
37. Lanzino G, Kongable GL, Kassell NF. Electrocardiographic abnormalities after nontraumatic subarachnoid hemorrhage. J Neurosurg Anesthesiol. 1994;6(3):156-62.
38. Khechinashvili G, Asplund K. Electrocardiographic changes in patients with acute stroke: a systematic review. Cerebrovasc Dis. 2002;14(2):67-76.
39. Fukui S, Katoh H, Tsuzuki N, et al. Multivariate analysis of risk factors for QT prolongation following subarachnoid hemorrhage. Crit Care. 2003;7(3):R7-R12.
40. Horowitz MB, Willet D, Keffer J. The use of cardiac troponin-I (cTnI) to determine the incidence of myocardial ischemia and injury in patients with aneurysmal and presumed aneurysmal subarachnoid hemorrhage. Acta Neurochir. 1998;140(1):87-93.
41. Bulsara KR, McGirt MJ, Liao L, et al. Use of the peak troponin value to differentiate myocardial infarction from reversible neurogenic left ventricular dysfunction associated with aneurysmal subarachnoid hemorrhage. J Neurosurg. 2003;98(3):524-8.
42. Naidech AM, Kreiter KT, Janjua N, et al. Cardiac troponin elevation, cardiovascular morbidity, and outcome after subarachnoid hemorrhage. Circulation. 2005;112(18):2851-6.
43. Zhang L, Wang Z, Qi S. Cardiac Troponin Elevation and Outcome after Subarachnoid Hemorrhage: A Systematic Review and Meta-analysis. J Stroke Cerebrovasc Dis. 2015;24(10):2375-84.
44. van der Bilt IA, Hasan D, Vandertop WP, et al. Impact of cardiac complications on outcome after aneurysmal subarachnoid hemorrhage: a meta-analysis. Neurology. 2009;72(7):635-42.
45. Masuda T, Sato K, Yamamoto S, et al. Sympathetic nervous activity and myocardial damage immediately after subarachnoid hemorrhage in a unique animal model. Stroke. 2002;33(6):1671-6.
46. Crago EA, Kerr ME, Kong Y, et al. The impact of cardiac complications on outcome in the SAH population. Acta Neurol Scand. 2004;110(4):248-53.
47. Tomida M, Muraki M, Uemura K, et al. Plasma concentrations of brain natriuretic peptide in patients with subarachnoid hemorrhage. Stroke. 1998;29(8):1584-7.
48. Pinnamaneni S, Dutta T, Melcer J, et al. Neurogenic stress cardiomyopathy associated with subarachnoid hemorrhage. Future Cardiol. 2015;11(1):77-87.
49. Tung PP, Olmsted E, Kopelnik A, et al. Plasma B-type natriuretic peptide levels are associated with early cardiac dysfunction after subarachnoid hemorrhage. Stroke. 2005;36(7):1567-9.
50. Sviri GE, Shik V, Raz B, et al. Role of brain natriuretic peptide in cerebral vasospasm. Acta Neurochir. 2003;145(10):851-60.
51. Yarlagadda S, Rajendran P, Miss JC, et al. Cardiovascular predictors of in-patient mortality after subarachnoid hemorrhage. Neurocrit Care. 2006;5(2):102-7.
52. Mayer SA, Lin J, Homma S, et al. Myocardial injury and left ventricular performance after subarachnoid hemorrhage. Stroke. 1999;30(4):780-6.
53. Zaroff JG, Rordorf GA, Ogilvy CS, et al. Regional patterns of left ventricular systolic dysfunction after subarachnoid hemorrhage: evidence for neurally mediated cardiac injury. J Am Soc Echocardiogr. 2000;13(8):774-9.
54. Dujardin KS, McCully RB, Wijdicks EF, et al. Myocardial dysfunction associated with brain death: clinical, echocardiographic, and pathologic features. J Heart Lung Transplant. 2001;20(3):350-7.
55. Banki NM, Kopelnik A, Dae MW, et al. Acute neurocardiogenic injury after subarachnoid hemorrhage. Circulation. 2005;112(21):3314-9.
56. Banki N, Kopelnik A, Tung P, et al. Prospective analysis of prevalence, distribution, and rate of recovery of left ventricular systolic dysfunction in patients with subarachnoid hemorrhage. J Neurosurg. 2006;105(1):15-20.
57. Khush K, Kopelnik A, Tung P, et al. Age and aneurysm position predict patterns of left ventricular dysfunction after subarachnoid hemorrhage. J Am Soc Echocardiogr. 2005;18(2):168-74.
58. Kothavale A, Banki NM, Kopelnik A, et al. Predictors of left ventricular regional wall motion abnormalities after subarachnoid hemorrhage. Neurocrit Care. 2006;4(3):199-205.
59. Sugimoto K, Watanabe E, Yamada A, et al. Prognostic implications of left ventricular wall motion abnormalities associated with subarachnoid hemorrhage. Int Heart J. 2008;49(1):75-85.
60. Hravnak M, Frangiskakis JM, Crago EA, et al. Elevated cardiac troponin I and relationship to persistence of electrocardiographic and echocardiographic abnormalities after aneurysmal subarachnoid hemorrhage. Stroke. 2009;40(11):3478-84.
61. Mayer SA, Fink ME, Homma S, et al. Cardiac injury associated with neurogenic pulmonary edema following subarachnoid hemorrhage. Neurology. 1994;44(5):815-20.
62. Kilbourn KJ, Levy S, Staff I, et al. Clinical characteristics and outcomes of neurogenic stress cadiomyopathy in aneurysmal subarachnoid hemorrhage. Clin Neurol Neurosurg. 2013;115(7):909-14.
63. Lee VH, Connolly HM, Fulgham JR, et al. Tako-tsubo cardiomyopathy in aneurysmal subarachnoid hemorrhage: an underappreciated ventricular dysfunction. J Neurosurg. 2006;105(2):264-70.
64. Mori H, Ishikawa S, Kojima S, et al. Increased responsiveness of left ventricular apical myocardium to adrenergic stimuli. Cardiovasc Res. 1993;27(2):192-8.
65. Zaroff JG, Pawlikowska L, Miss JC, et al. Adrenoceptor polymorphisms and the risk of cardiac injury and dysfunction after subarachnoid hemorrhage. Stroke. 2006;37(7):1680-5.
66. Nanda S, Bhatt SP, Dale TH. Tako-tsubo cardiomyopathy: an insight into pathogenesis. Chest. 2008;133(2):583.
67. Villareal RP, Achari A, Wilansky S, et al. Anteroapical stunning and left ventricular outflow tract obstruction. Mayo Clin Proc. 2001;76(1):79-83.
68. Bybee KA, Kara T, Prasad A, et al. Systematic review: transient left ventricular apical ballooning: a syndrome that mimics ST-segment elevation myocardial infarction. Ann Intern Med. 2004;141(11):858-65.
69. Sharkey SW, Lesser JR, Zenovich AG, et al. Acute and reversible cardiomyopathy provoked by stress in women from the United States. Circulation. 2005;111(4):472-9.