
{kind=link}
| Author | Affiliation |
|---|---|
| Philip D. Nibley, MD | Vituity Emergency Medicine, Sacramento, California |
| Chadd K. Kraus, DO, DrPH, MPH | Geisinger Health, Department of Emergency Medicine, Danville, Pennsylvania |
Introduction
Case report
Discussion
Conclusion
ABSTRACT
We present a case report and review of the literature of rib osteomyelitis in a pediatric patient presenting to the emergency department (ED) with fever and increased work of breathing. The patient was seen on a return visit to the ED after discharge with presumed viral illness approximately 12 hours prior. On the second ED visit, there was concern for occult bacteremia, and work-up ultimately revealed a subperiosteal abscess with rib osteomyelitis, a rare etiology for fever in the pediatric patient. The patient was treated with antibiotics, had surgical debridement, and fully recovered.
INTRODUCTION
Fever is a common presenting complaint of pediatric patients in the emergency department (ED). Fever can represent non-specific viral syndromes or serious bacterial infections. Occult bacterial infections, such as osteomyelitis, are less common than viral infections but can frequently elude diagnosis. We present a case report and review of the literature of rib osteomyelitis in a pediatric patient presenting to the ED with fever and increased work of breathing.
CASE REPORT
A nine-month-old male presented to the ED with a four-day history of fever and increased work of breathing. He was first seen by his primary care physician with the onset of symptoms. His mother later took him to the ED where he had a fever but no respiratory distress. He was treated symptomatically and discharged with presumptive diagnosis of viral illness. He returned to the ED approximately 12 hours after discharge with abdominal pain and recurrence of his fever. His parents noted that the patient seemed to be in pain and had grunting with expiration. He also had decreased oral intake, but was still making wet diapers.
His parents also reported cyclical periods of crying during which he seemed uncomfortable. They noted that he seemed to be pale with decreased energy and activity from baseline. Mom also reported no bowel movements for the prior 24 hours, with the patient normally having 2–3 bowel movements daily. Parents denied any cough, congestion, wheezing, stridor, vomiting, or rash. He had no past medical history, and his vaccinations were up to date.
On exam the patient had a rectal temperature of 101.5 degrees Fahrenheit, heart rate of 187 beats per minute, respiratory rate of 36 breaths per minute, and oxygen saturation of 99% on room air. He appeared to be developmentally appropriate and in moderate distress with pale skin; he exhibited no cyanosis, rash, or lesions. He had an expiratory grunt with each breath. No cardiac murmur was appreciated and the lungs were clear without wheezes. The abdomen revealed no focal tenderness. Muscle tone was within normal limits. His neurological exam was without focal deficits and age appropriate.
Labs showed a white blood cell count of 17.0 K/microliter (mcL) (normal 6.0–17.5 K/mcL), C-reactive protein of 13.16 milligrams per deciliter (mg/dL) (normal 0–0.80 mg/dL), lactic acid of 1.8 millimoles/L. Urinalysis was unremarkable. The chest radiograph and ultrasound of the abdomen were unremarkable. An electrocardiogram showed sinus tachycardia. Blood cultures were ordered and the patient was started on empiric antibiotics (piperacillin/tazobactam) in discussion with the pediatric hospitalist service. He was admitted for additional evaluation of fever of unknown origin. Blood cultures were initially positive for methicillin-susceptible Staphylococcus aureus (MSSA). An echocardiogram ordered for suspicion of endocarditis was normal. Antibiotics were continued, and the patient improved clinically; however, his parents noted during his hospitalization that he seemed to be in pain when he was picked up, particularly in his axillae.
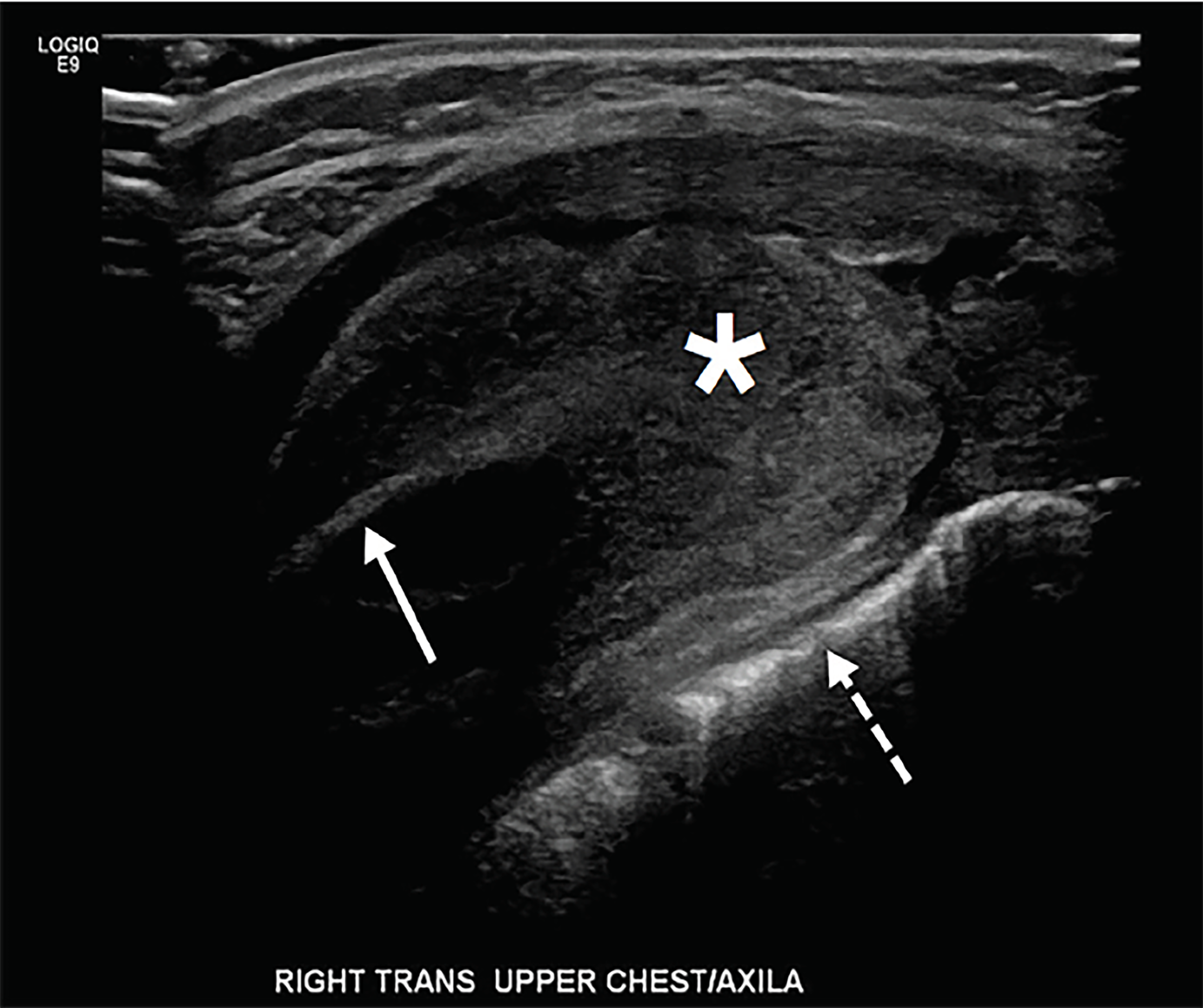
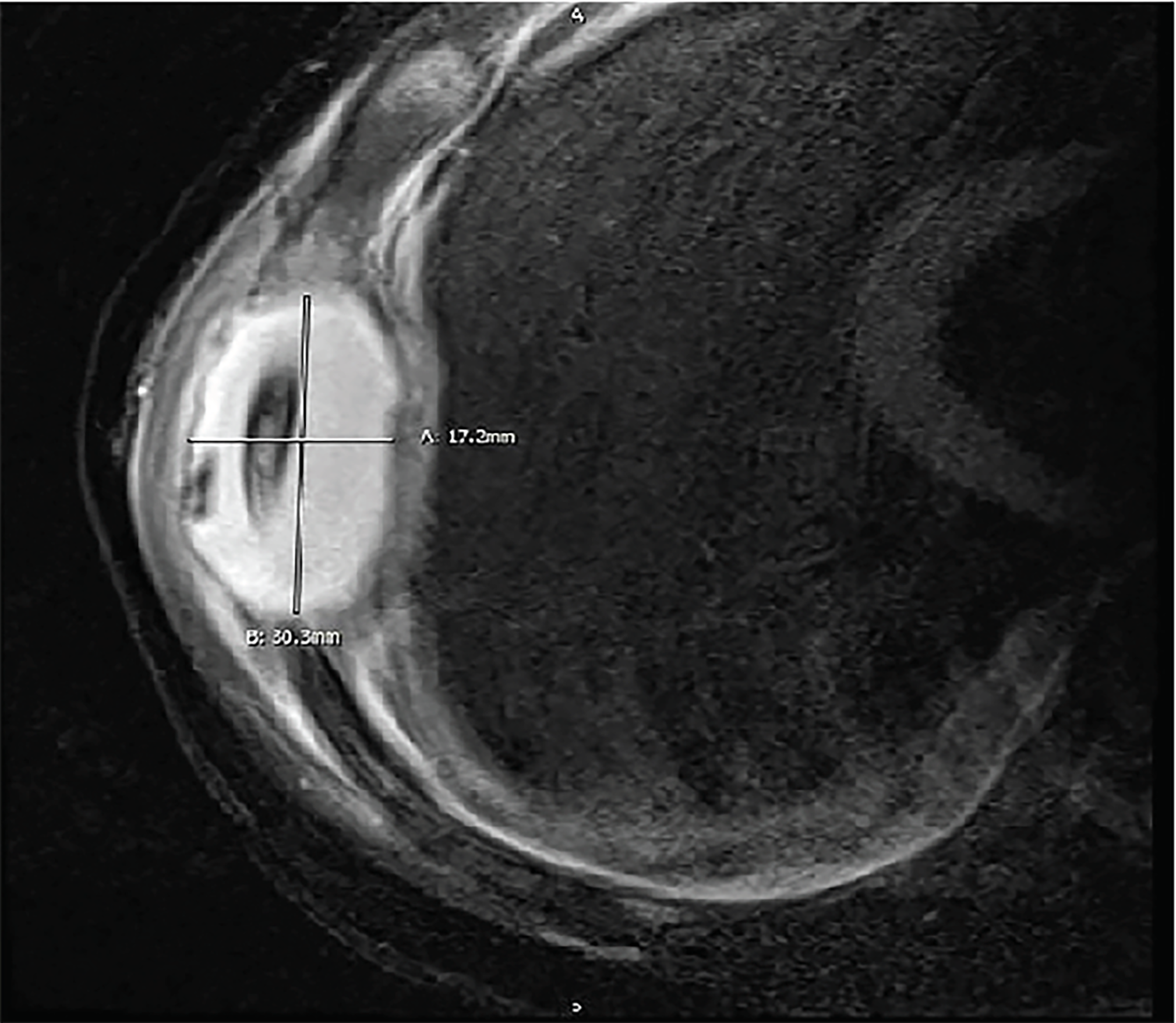
Repeat blood cultures obtained after antibiotic therapy were negative, and the patient’s fevers were less frequent. He was transitioned to oral cephalexin and observed. On hospital day six, the patient’s mother noted a 2×4 centimeter tender, non-erythematous mass in the right axilla. Formal ultrasound showed a soft tissue mass adjacent to the rib, without a definitive fluid collection (Image 1). The patient was transferred to a specialized pediatric hospital where magnetic resonance imaging (MRI) revealed that the axillary mass was consistent with osteomyelitis and subperiosteal abscess of the lateral seventh rib (Image 2). The patient had operative debridement and thereafter made a full recovery with discharge home on hospital day 12.
DISCUSSION
Rib osteomyelitis in pediatric patients is rare, with less than 60 cases reported in the literature.1,3 It has been described in association with tuberculosis,4 via hematogenous spread,5 and as a sequela of child abuse.6 Our case illustrates that uncommon and rare causes of fever of unknown origin, such as osteomyelitis, should be considered in the evaluation of pediatric patients presenting to the ED. The etiology of osteomyelitis in this case was not clear, and could have been the result of hematogenous spread, although no primary site of infection was evident. Most cases of rib osteomyelitis are S. aureus,2,7,8 although other organisms including Streptococcus pneumonia and Group A beta hemolytic Streptococcus have also been implicated.9-11
CPC-EM Capsule
What do we already know about this clinical entity?
In pediatric patients presenting to the emergency department (ED) with fever, occult bacterial causes, such as osteomyelitis, are less common than viral causes but frequently elude diagnosis.
What makes this presentation of disease reportable?
Rib osteomyelitis in pediatric patients is rare, with less than 60 cases reported in the literature.
What is the major learning point?
The diagnosis of rib osteomyelitis requires a high index of suspicion by the emergency physician, especially because the presentation can be non-specific.
How might this improve emergency medicine practice?
Uncommon and rare causes of fever of unknown origin, such as osteomyelitis, should be considered in the evaluation of pediatric patients presenting to the ED.
CONCLUSION
The diagnosis of rib osteomyelitis requires a high index of suspicion by the emergency physician, especially because the presentation can be non-specific2 as in the case presented. Definitive diagnosis often requires advanced imaging such as computed tomography or MRI, or invasive testing such as biopsy or aspiration with culture, although ultrasound12 and plain radiography13 are potentially useful in the initial evaluation. As in the case presented, ultrasound has some role in identifying subperiosteal abscess.14
Documented patient informed consent and/or Institutional Review Board approval has been obtained and filed for publication of this case report.
Footnotes
Section Editor: Rick A. McPheeters, DO
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
Address for Correspondence: Chadd K. Kraus, DO, DrPH, MPH, Geisinger Health, Department of Emergency Medicine, MNC:20-05, 100 North Academy Avenue, Danville, PA 17822. Email: chaddkraus@gmail.com. 2:294 – 296
Submission history: Revision received June 26, 2018; Accepted September 6, 2018
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. At the time the manuscript was drafted, Dr. Nibley was an emergency medicine resident at WellSpan Health – York Hospital in York, Pennsylvania.
REFERENCES
1. Idrissa S, Tazi M, Cherrabi H, et al. Multifocal rib osteomyelitis in children: a case report and literature review. J Surg Case Rep. 2017;2017(7).
2. Nascimento M, Oliveira E, Soares S, et al. Rib osteomyelitis in a pediatric patient case report and literature review. Pediatr Infect Dis J. 2012;31(11):1190-4.
3. Donovan RM, Shah KJ. Unusual sites of acute osteomyelitis in childhood. Clin Radiol. 1982;33(2):222-30.
4. Kashyap NK, Jindal A, Borkar NK, et al. Primary tuberculotic osteomyelitis of rib in a child. J Clin Diagn Res. 2017;11(7):PD08-PD09.
5. Annen MJ, Johnston MJ, Gormley JP, et al. Acute hematogenous osteomyelitis presenting as a “cold” rib in a child. World J Nucl Med. 2017;16(2):160-2.
6. Ribe JK, Changsri C. A case of traumatic osteomyelitis in a victim of child abuse. Am J Forensic Med Pathol. 2008;29(2):164-6.
7. Basa NR, Si M, Ndiforchu F. Staphylococcal rib osteomyelitis in a pediatric patient. J Pediatr Surg. 2004;39(10):1576-7.
8. Goergens ED, McEvoy A, Watson M, et al. Acute osteomyelitis and septic arthritis in children. J Paediatr Child Health. 2005;41(1–2):59-62.
9. Ibia EO, Imoisili M, Pikis A. Group A beta-hemolytic streptococcal osteomyelitis in children. Pediatrics. 2003;112(1 Pt 1):e22-6.
10. Naik-Mathuria B, Ng G, Olutoye OO. Lytic rib lesion in a 1-year-old child: group A beta streptococcal osteomyelitis mimicking tumor. Pediatr Surg Int. 2006;22(10):837-9.
11. Kalouche I, Ghanem I, Kharrat K, et al. Osteomyelitis of the rib due to Streptococcus pneumoniae: a very rare condition in children. J Pediatr Orthop B. 2005;14(1):55-60.
12. Emiley PJ, Kendall JL, Bellows JW. Acute hematogenous osteomyelitis of the rib identified on bedside ultrasound. J Emerg Med. 2015;48(1):e15-7.
13. Bar-Ziv J, Barki Y, Maroko A, et al. Rib osteomyelitis in children. Early radiologic and ultrasonic findings. Pediatr Radiol. 1985;15(5):315-8.
14. Wright NB, Abbott GT, Carty HM. Ultrasound in children with osteomyelitis. Clin Radiol. 1995;50(9):623-7.