
{kind=link}
| Author | Affiliation |
|---|---|
| Ali Pourmand, MD, MPH | George Washington University, Department of Emergency Medicine, Washington, DC |
| Keith Boniface, MD | George Washington University, Department of Emergency Medicine, Washington, DC |
ABSTRACT
Introduction:
Emergency ultrasound is now used in both community and academic hospitals for rapid diagnosis and treatment of life-threatening conditions. Bedside emergency echocardiography can rapidly identify significant pathology such as pericardial effusions and tamponade, right ventricle dilatation due to pulmonary embolism, and cardiac hypokinesis, and aid in the diagnosis and management of patients in emergency department (ED).
Case Report:
A 41-year-old man presented twice to the ED with history of abdominal pain and was diagnosed with primary cardiac angiosarcoma with point-of-care ultrasound.
Conclusion:
This case is illustrative of how bedside cardiac ultrasound in the ED can dramatically change a patient’s hospital course.
INTRODUCTION
Bedside emergency ultrasound is a modality that can expedite diagnosis, change management, and facilitate disposition in the emergency department (ED). The use of emergency ultrasound is now disseminated in both community and academic hospitals for rapid diagnosis and treatment of life-threatening conditions. We present a case of a patient with abdominal pain in which bedside ultrasound dramatically changed a patient’s hospital course.
CASE REPORT
A 41-year-old African-American man initially presented to the ED after 2 weeks of subacute generalized abdominal pain. His initial workup included a complete blood count, chemistries, a liver panel, and a lipase level, all within normal limits. He also underwent computed tomography (CT) scanning of the abdomen and pelvis, which showed a 3.0-cm mass in the right hepatic lobe with peripheral ring enhancement during the arterial phase, interpreted by radiology as consistent with a cavernous hemangioma. The patient was discharged with a diagnosis of abdominal pain, given a prescription for a proton-pump inhibitor, and instructed to follow up as an outpatient with the medical clinic. One week later, the patient returned to the ED, complaining of continued generalized crampy abdominal pain with no relief from the proton-pump inhibitor. He also complained of mild nausea without vomiting, urinary symptoms, fever, or trauma. He had no significant medical history or family history. Social history was significant for smoking and occasional alcohol use. Initial vital signs were as follows: blood pressure, 125/78, pulse, 80; respiratory rate, 14; O2 saturation of 98% on room air; temperature, 98.7°F. On physical examination, the cardiac examination was normal. The abdomen was soft, with generalized tenderness to palpation, but no guarding, rebound, or signs of an acute abdomen were elicited. The remainder of the physical examination was normal.
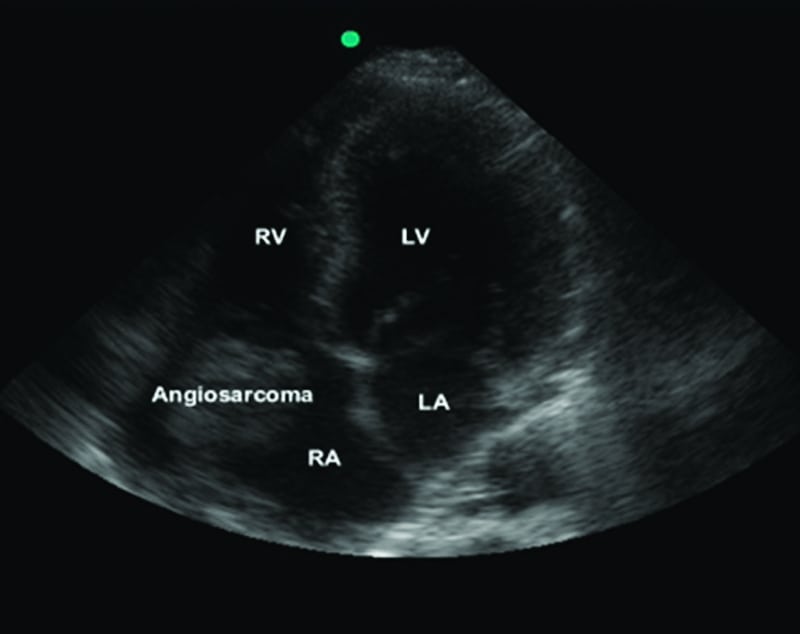
At this juncture, given the normal results of laboratory and radiologic testing from the prior visit, a bedside ultrasound was performed of the right upper quadrant, heart, and abdomen, by using a Sonosite Micromaxx with a 5- to 2-MHz phased-array transducer (Sonosite, Bothell, Washington). The initial indication for the use of bedside ultrasound was to search for biliary disease and free intra-abdominal fluid in this patient with abdominal pain and a prior normal abdominal CT scan. The right upper quadrant examination demonstrated a normal gallbladder, and the Focused Assessment with Sonography in Trauma (FAST) examination was without free fluid. A view of the heart was included as the fourth view of the FAST examination, and the cardiac images revealed a 5-cm hyperechoic mass in right atrium that appeared to be tethered to the free atrial wall (Figure 1). After this finding, cardiology and cardiothoracic surgery were consulted, and the patient was admitted to the cardiovascular service. A chest CT and repeated abdominal CT scan were performed. The chest CT demonstrated a well-circumscribed 4-cm filling defect in the right atrium, with possible extension into the right ventricle. No evidence of pulmonary embolism was seen in the right or left main pulmonary arteries or in any of the visualized branches. The abdominal CT demonstrated the 3-cm hypodense mass, seen on the prior CT scan, in the right lobe of the liver. The differential diagnosis reported by radiology for this examination was hemangioma versus metastasis. The patient underwent surgery with radical resection of the right atrial wall tumor and reconstruction of the right atrial wall with a large piece of autogenous pericardium (Figure 2). After histopathologic evaluation, tumor features were found to be typical for cardiac angiosarcoma, spindle-cell type.

DISCUSSION
Point-of-care echocardiography skills can rapidly identify life-threatening pathology, and aid in the diagnosis and management of patients in ED.1,2 These findings can at times dramatically change patient disposition. In the case presented, an ultrasound looking for biliary disease and free fluid in the abdomen was extended to include the heart. The echocardiogram revealed the presence of a cardiac mass that had gone undetected on the prior visit, and would probably have otherwise gone undetected on the second visit.
The majorities of primary cardiac tumors (approximately 75%) are benign, most commonly atrial myxomas.3,4 Cardiac angiosarcoma is the most common malignant tumor of the heart, and two thirds of angiosarcomas are located in the right side of the heart, especially the atrium. These tend to present with chest pain, cough, syncope, or dyspnea in young and middle-aged patients.5,6 Cardiac angiosarcomas can also remain an asymptomatic tumor until they metastasize. Extracardiac manifestations, including abdominal pain, can occur with intracardiac tumors. In a case reported by McCoskey et al,7 a 37-year-old woman with persistent abdominal pains and nausea actually underwent diagnostic laparoscopy 5 weeks before eventually being diagnosed with an atrial myxoma.
In our case, a patient with an intracardiac tumor had a similarly unusual clinical presentation with abdominal pain as his predominant symptom. His abdominal pain could have resulted from hepatic congestion from right-sided obstruction to cardiac flow (although the liver-function tests were normal on both visits), indirectly through autoimmune causes, or directly from his hepatic mass. This presentation is different from the typical pattern of pulmonary emboli, pulmonary hypertension, and vena cava obstruction found with intracardiac tumors.4,8
CONCLUSION
Bedside echocardiography is a rapidly accessible, low-cost, noninvasive procedure that greatly benefitted this ED patient. This case illustrates how ED point-of-care ultrasound dramatically changed the disposition in a case that was initially being tracked toward outpatient follow-up. Beyond pericardial effusion, bedside echocardiography is able to identify other cardiac pathology such as intracardiac masses. Emergency providers should have a low threshold for the use of bedside cardiac ultrasound.
Footnotes
Supervising Section Editor: Seric S. Cusick, MD
Submission history: Submitted March 13, 2010; Revision received September 13, 2010; Accepted April 11, 2011
Reprints available through open access at http://escholarship.org/uc/uciem_westjem
DOI: 10.5811/westjem.2011.4.1906
Address for Correspondence: Ali Pourmand, MD, MPH
George Washington University, 2150 Pennsylvania Ave NW, Ste 2B, Washington, DC 20037
E-mail: pourmanda@yahoo.com
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Wright J, Jarman R, Connolly J, et al. Echocardiography in the emergency department. Emerg Med J. 2009;;26:82–86. [PubMed]
2. Tang A, Euerle B. Emergency department ultrasound and echocardiography. Emerg Med Clin North Am. 2005;;23:1179–1194. [PubMed]
3. Vander Salm TJ. Unusual primary tumors of the heart. Semin Thorac Cardiovasc Surg.2000;;12:89–100. [PubMed]
4. Chidel MA, Macklis RM. Perez C, LW Brady, Halperin EC, et al., editors. Tumors of the heart and great vessels. Principles and Practice of Radiation Oncology. Philadelphia, PA: Lippincott Williams and Wilkins. 2004. pp. 1305–1314.
5. Naka N, Ohsawa M, Tomita Y, et al. Angiosarcoma in Japan: a review of 99 cases. Cancer.1995;;75:989–996. [PubMed]
6. Reece IJ, Cooley DA, Frazier OH, et al. Cardiac tumors: clinical spectrum and prognosis of lesions other than classical benign myxoma in 20 patients. J Thorac Cardiovasc Surg. 1984;;88:439–446.[PubMed]
7. McCoskey EH, Mehta JB, Krishnan K, et al. Right atrial myxoma with extracardiac manifestations.Chest. 2000;;118:547–549. [PubMed]
8. Fortmann T. Hemorrhagic nonspecific pericardial effusion as an initial symptom of angiosarcoma of the right heart. Z Kardiol. 2004;;93:807–812. [PubMed]