
{kind=link}
| Author | Affiliation |
|---|---|
| Kenneth A. Corre, MD | Cedars-Sinai Medical Center, Ruth and Harry Roman Emergency Department, Los Angeles, CA |
| Alissa Arnold, BS | Cedars-Sinai Medical Center, Ruth and Harry Roman Emergency Department, Los Angeles, CA |
ABSTRACT
Introduction:
This case report describes a digit amputation resulting from an improperly applied tubular dressing. The safe application of digital tubular dressings, and the rationale behind it, is detailed to raise emergency physician (EP) awareness.
Methods:
We present a case report of a recent iatrogenic-induced digit ischemia caused by improperly applied tube gauze. We review the literature on the subject and the likely sources of poor outcomes presented. The proper application of tubular gauze dressings is then outlined.
Conclusion:
EPs and emergency department personnel must be educated on the safe application of tubular gauze dressings to avoid dire outcomes associated with improper applications.
INTRODUCTION
Since their introduction in the mid-1950s, tubular gauze dressings have been commonly applied to the digits in emergency departments (ED), urgent care, office and other surgical settings. The dressing, also available online for purchase by the public, is placed over a metal or plastic cage and then slipped over the digit in successive layers. Package inserts offer incomplete details on the proper application. The use of tubular gauze dressings is safe when applied methodically and properly. However, the potential for disaster exists when they are improperly placed. This paper presents a case report of iatrogenic digital compromise resulting in amputation, reviews the literature on this topic, and presents the proper application of tube gauze and the anticipated dangers associated with its improper use.
CASE
A 10-year-old girl reached into a compact car parked on a grade. As she removed her right hand, the door closed under the pull of gravity and caught her left fifth digit. She presented to the emergency department (ED) with a superficial non-suturable laceration over the dorsal distal inter-phalangeal joint. Neuro-vascular-motor-tendon functions were normal, capillary refill was under three seconds, and x-rays were negative. The wound was prepped and Spandage® (Medi-Tech International Corporation, Brooklyn, NY) tubular finger gauze was applied. Although the child experienced increased pain after the dressing application, the exact manner of application was unknown. The discharge diagnosis was “5th digit superficial laceration.”
Follow up within 72 hours was instructed. At that time, digit ischemia was noted and plastic surgery was consulted. The zone of ischemia was allowed to demarcate over several weeks and the digit was eventually amputated at the proximal inter-phalangeal joint (PIP). The child had no underlying co-morbidity that would make her more susceptible to ischemia from an improperly applied dressing.
DISCUSSION
In 1975 four cases of digital ischemia associated with the use of digital tubular gauze were reported in the literature.1 Each involved a superficial injury to a different digit and was dressed with a Surgifix® (BSN Medical) tubular plastic net bandage in place of the “older” dressing material, Tubgauz® (Scholl). Three of the dressings were found to be “constrictive” at the base of digits on follow-up. One required amputation, while the other three recovered completely. The constriction at the base of two of the digits was relegated to a “twist” in the bandage in that area during dressing application. The authors hypothesized that Surgifix® is more elastic and coarser than the fine meshed Tubegauz® and becomes a constrictive tourniquet when twisted in multilayers.
In 1982 a 16-year-old boy amputated half of his distal phalanx.2 After repair the remaining finger was dressed in multiple layers with an elastic net bandage. Four days post-op the patient had unexpected pain in the injured digit and the rest of the finger required amputation. The author measured the amount of pressure exerted by multiple layers of an elastic net bandage as compared to the cotton tube gauze. Each layer of elastic net produced increasing tension in the next layer and this effect was dramatic, cumulative, and potentially constrictive. This was not the case with the cotton tube gauze.
In 1986 a case report documented a 21-year-old with a severe crush injury to the distal tip of his right middle finger associated with a comminuted distal tuft fracture.3Neurovascular-tendon function was intact. The nail was removed and lacerations were repaired followed by seven layers of an elastic tubular dressing. The patient’s finger became severely painful and the tubular bandage was noted to be “tight.” The finger was eventually amputated. The author concluded that more than two layers of dressing should be avoided, especially when the elasticized bandages are used. Twisting of the proximal end of the dressing should either be avoided or limited to less than 90-degree arc. Every patient should be cautioned to remove the dressing and return if severe, throbbing pain develops or if the digit swells despite elevation.
In 1995 a 54-year-old underwent the elective excision of a benign cyst from the nail fold of a digit. A tubular gauze dressing was applied in three layers, each with a 90-degree twist over a thin contact dressing. A non-circumferential adhesive tape was applied proximally to secure the dressing. The patient returned for a wound check 18 hours later and, although the dressing was noted to be “unusually tight,” the patient was asymptomatic and the digit “appeared normal.” The patient was re-examined three hours later due to pain. The digit was found to be cyanotic under the dressing. Gradual, full recovery occurred. The investigators measured the effects of different types of tubular gauze applications and found that the following techniques produced increasing pressure and constriction in the following order: three layers, 90-degree twist < three layers, 540 degree twist < rolled proximal edge < excess longitudinal traction < five layers, 90-degree twist. Twisting and traction referred to maneuvers undertaken during on-the-digit application. The absence of pain immediately after the dressing application was not reassuring.
In 2005 an afebrile 74-year-old woman smoker, with hypertension, type II diabetes, and hyperlipidemia presented to the ED with a finger paronychia.4 Incision and drainage was followed by tube gauze applied in “standard fashion.” The gauze used appeared to be of the elastic Spandage® variety. She was discharged on Keflex® which she started two days late. She returned to the ED on day 5 and the dressing was noted to be tight. The finger was found to be discolored, dusky and indurated from the PIP forward and required eventual amputation.
In the current case we present, the overwhelming likelihood is that the tubular dressing was misapplied and produced ischemia and the dire surgical result. The mechanism and force of injury were relatively minor and could not reasonably be expected to account for the final consequence. As well, the injury forces were applied to the anterior and posterior aspects of the distal digit, not bi-laterally where the vessels lie. Properly applied tubular gauze is likely very safe: cotton gauze loaded onto a cage inserted over the digit and unloaded onto the digit as the cage is moved proximally to distally in two layers or less. However, any misapplied tubular dressing, be it by twisting and/or axial traction of the dressing on the digit, and/or multilayers, is a set up for profound morbidity. When twisted, the normal mesh, which usually serves to evenly distribute minor pressure with minimal to no constriction, becomes rope-like and can act as a tourniquet. When axial or longitudinal traction is applied, significant constriction may occur, but over a much wider area. These constrictive forces are mechanically intuitive and borne out in the literature.
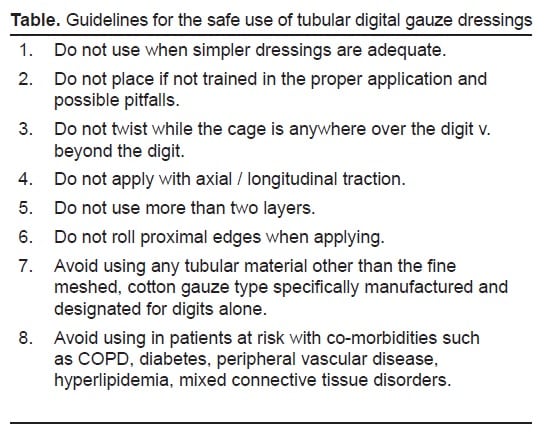
Substituting coarser and more elastic materials in place of the intended cotton finger tubular gauze further increases the potential for danger. Indeed, one elastic manufacturer currently cautions in its application procedures and directions that one should never apply more than two layers to any dressed appendage.5 Likewise, tubular gauze dressings should be avoided if possible in those with co-morbidities that result in underlying vascular compromise. The table outlines our recommended proper use of tube gauze to avoid constrictive dressings and bad outcomes on digits.
CONCLUSION
The dangers of improper applications of various types of tubular gauze to digits have been known for at least three decades. Yet the contemporary case report presented here details a severe and unacceptable consequence to tubular gauze application.
Footnotes
Supervising Section Editor: H. Bryant Nguyen, MD, MS
Submission history: Submitted April 29, 2008; Revision Received December 18, 2008; Accepted December 19, 2008
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Ken Corre, MD. Department of Emergency Medicine, Cedars-Sinai Medical Center, 8700 Beverly Blvd., Los Angeles, CA 90048
Email: Kenneth.Corre@cshs.org
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Miller TA, Haftel AJ. Iatrogenic digital ischemia. West J Med. 1975;122:183–4.[PMC free article] [PubMed]
2. Ersek RA. Ischemic necrosis and elastic net bandages. Tex Med. 1982;78:47–9.[PubMed]
3. Neal JM. Iatrogenic digital ischemia. Ann Emer Med. 1986;15:382–3.
4. Norris RL, Gilbert FH. Digital necrosis necessitating amputation after tube gauze dressing application in the ED. Amer J Emer Med. 2005;12:619–21.
5. Application procedures for cut to fit original spandage & mt-spandage. Brooklyn, NY: Medi-Tech International Corporation; 2001. Available at: http://www.medi-techintl.com/app_procedure.pdf Accessed July 6, 2009.