
{kind=link}
| Author | Affiliation |
|---|---|
| Julie Gorchynski, MD | CHRISTUS Spohn Memorial Hospital, Texas A&M, Department of Emergency Medicine |
| John Herrick, DO | CHRISTUS Spohn Memorial Hospital, Texas A&M, Department of Emergency Medicine |
| Edgar Cortes, MD | Driscoll Children’s Hospital, Department of Pediatric Emergency Medicine |
ABSTRACT
Acute ischemic stroke in a pediatric patient is a complex disease with a variety of etiologies that differ from adults. Though rare, they are a real phenomenon with potentially devastating consequences. Some treating institutions are using anti-thrombotic drug therapy with unclear benefits. Available literature, which is limited to case reports and retrospective reviews of databases, clouds this topic with both positive and negative outcomes. Emergency department management should focus on stabilization and resuscitation with immediate involvement of a pediatric neurologist and intensivist. The decision to use anti-thrombotic drug therapy, including anti-platelet drugs and thrombolytics, should be in consult with the specialists involved until randomized controlled trials determine their safety and efficacy in the pediatric population.
INTRODUCTION
Acute ischemic stroke (AIS) in a pediatric patient is a rare medical emergency with an incidence of only 2–3 per 100,000.1 Cognitive and behavioral sequelae frequently arise with social implications and effects on daily living.2 The etiologies of stroke in a child are more varied than in adults and are not always due to acute clot formation or hemorrhage. Literature on this topic, including the use of anti-thrombotic therapy for children presenting with AIS, is sparse. Studies in the adult population show anti-thrombotic drugs, including aspirin, are effective when administered using recommended guidelines.3 The role of thrombolytics is controversial with conflicting evidence. 4,5,6 This case report describes an 11-year-old boy who presented to the emergency department (ED) of a small rural community with the diagnosis of an acute ischemic stroke. After transfer to a children’s hospital and an exhaustive workup, the etiology of his stroke remained unclear. At four-month outpatient follow-up, the patient had only minimal left arm weakness. Background information on AIS in the pediatric population is presented, including ED management and the role of anti-thrombotic drug therapy.
CASE
An 11-year-old Hispanic male presented to the ED 30 minutes after the sudden onset of headache, left-sided weakness and dysarthria. His vital signs were within normal limits. Left arm and leg strength were 2/5 with a noticeable facial droop. Cardiac exam showed a regular rate and rhythm with no murmurs. Chest was clear and abdomen was soft. No petechiae were noted on his skin. Fingerstick blood glucose was normal. A CT scan of the head showed edema to the right frontal lobe without evidence of hemorrhage. Transfer for higher level of care was initiated with the presumptive diagnosis of acute ischemic stroke. A long transport time placed him at the nearest children’s hospital eight hours after symptom onset. An emergent MRI showed findings consistent with a right frontal lobe and basal ganglia ischemic infarction (Figure 1). The patient was given aspirin, empiric intravenous antibiotics and antiviral medications in the ED. A thorough work-up ensued in the pediatric intensive care unit. An MRA of the brain, carotid Doppler and echocardiogram were normal. The lumbar puncture, ECG, CBC, chemistry panel, liver enzymes, cardiac enzymes and urine drug screen were normal, as were the SLE panel, Protein C and S, Factor V Leiden, anti-phospholipid antibodies, anti-thrombin III and coagulation profile, metabolic screening tests, blood and CSF cultures. The patient remained stable for the first two days and regained some motor strength. His hospital stay was complicated by a worsening headache. The CT demonstrated increased intracranial pressure that resolved following treatment with mannitol and steroids. After four weeks of extensive testing and rehabilitation, the etiology for his ischemic stroke remained elusive. The patient expended significant time and effort with a physical therapist. Upon discharge, he had regained the ability to walk and was able to move his left arm above his head. At his four-month follow-up, he had mild residual left arm weakness with no deficits in his gait or speech.
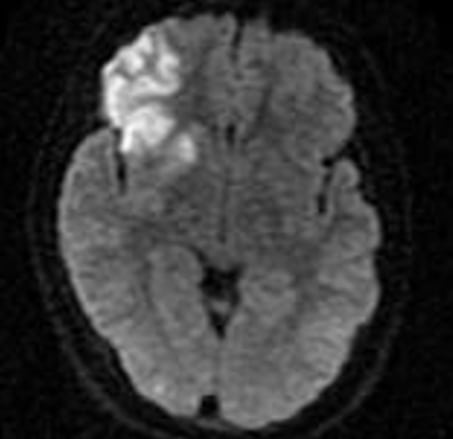
Diffusion Weighted MRI consistent with a right frontal lobe and basal ganglia ischemic infarction
DISCUSSION
AIS in a pediatric patient is defined as a stroke occurring between the ages of one month and 18 years. This relatively rare condition varies geographically with occurrence in the United States at 2–3 per 100,000 patients.1 By contrast, the overall incidence rate for total stroke (first-ever and recurrent of all ages) was 269 per 100,000 population.7Eighty percent of adult strokes are due to ischemia. While ischemic strokes in adults are usually thrombotic or embolic in nature, they may also be caused by hypoperfusion states. Cryptogenic strokes comprise 30 to 40% of all adult ischemic strokes and approximately 50% in children.2,8
Acute ischemic strokes in children most commonly occur between the ages of 1–5 years and least commonly in the extremes (< 1 year and > 15 years).9 Focal neurological signs occur in three-quarters of patients, with hemiplegia the most common.9 Despite the fact that infection accounts for 26% of cases, fever is present only 11% of the time.9 The risk factors for stroke in children are congenital heart disease, infection, prothrombotic disorders, trauma, acquired and congenital vascular disease, sickle cell disease, metabolic disorders and mitochondrial disease.9 Vascular disease alone accounts for one-third of cases, while metabolic disorders and prothrombotic disorders comprise 18% and 13% of cases respectively.9 Trauma makes up an additional 11% of cases.9 At least one risk factor is present in 90% of patients with almost 25% of patients having more than one.9
There appears to be demographic variation with a predilection for both gender and ethnicity. A seasonal variation may exist, as the disease most commonly occurs during the summer and least commonly during the winter.9 African-Americans have a significantly higher risk of suffering from both ischemic stroke and hemorrhagic strokes.10 Males carry a significantly higher risk of suffering all stroke subtypes compared to females.10
ED management of a child suffering from an ischemic stroke should focus on stabilization and transfer to an appropriate facility for specialty care. Stabilization begins with securing the airway, providing supplemental oxygen, establishing IV access and monitoring vitals signs and mental status. An emergent CT of the head in the ED should not be delayed. An ECG, CXR and lab work should be sent, including a complete blood count, blood and CSF cultures, chemistry, liver enzymes, cardiac markers, coagulation factors, urine analysis and urine drug screen. Empiric intravenous antibiotics and antivirals, maintenance fluid with an isotonic, non-dextrose containing fluid must be initiated in the ED.
Anti-platelet drugs are widely used in adults after literature has shown they reduce the rate of strokes.2 Although randomized controlled trials with children have not been conducted, anti-platelet drugs are used in some centers to reduce the recurrence rate of stroke.2 Adverse effects, such as severe bleeding or the precipitation of Reye’s syndrome, are rare.2 The use of anti-thrombotic drugs remains controversial in the pediatric literature and is not the standard of care.3 However, anti-thrombotic drugs are being given to pediatric patients at some institutions despite a paucity of supporting literature. The benefits are unclear, and it seems their use is based on adult studies, case reports and expert opinion.11 One study showed 1.6% of pediatric AIS patients admitted between 2000 and 2003 received thrombolytic therapy.1 The children receiving thrombolytics had significantly higher medical costs, were less likely to be discharged home and had higher overall mortality rates.1 Shortcomings of these findings were noted, including the small sample size and unknown severity of any of the patients at the time of presentation. Conversely, several case reports have been published showing potential benefits using thrombolytic therapy in children, including success stories across a wide age range and administration of thrombolytics well outside of the standard three-hour window used in adults.11,12
There are numerous etiologies for acute ischemic stroke in the pediatric population. Arterial dissection is one important cause. While most dissections occur in the internal carotid artery, children may dissect intracranially. MRI and contrast MRA show the anatomy without the risks of traditional angiography or radiation. Duplex ultrasonagraphy is useful, but CT angiogram still remains the gold standard for further investigation for suspected arterial dissection.13 Secondly, cerebral venous sinus thrombosis may cause strokes in children. This commonly develops from extension of infections, including acute otitis media, mastoiditis, pharyngitis, sinusitis, or meningitis. If infection is suspected, appropriate intravenous antimicrobials to include a third-generation cephalosporin, vancomycin and acyclovir should be initiated. Additionally, infectious vasculitis may occur from chronic infections such as tuberculous meningitis or rickettsial infection. Vasculitis may also be seen with common viral illnesses such as varicella and coxsackie. Lastly, cerebral vasculitis should be considered in children with either ischemic or hemorrhagic stroke, as well as strokes associated with fever or rash.13While erythrocyte sedimentation rate may be used as a screening tool, its interpretation should be used with caution since it does not exclude all vascular etiologies for ischemic stroke. There is no literature to support the empiric use of steroids; however, they may be given to treat cerebral edema or a vasculitic cause of stroke.
The rate of recurrence for childhood stroke may be as high as 30% and is dependent upon the etiology of the stroke.2 Children with a hypercoagulable disorder or a vascular diagnosis have a higher likelihood of recurrent stroke. Sickle cell disease patients have a 40% chance of repeat stroke, while children with arterial dissection have a recurrence rate of 12%.13
Children who suffer AIS generally recover better than adults, but the effects may still be long lasting and detrimental.14 While children who suffer a stroke have good educational and mobility outcomes, they have poorer outcomes when it comes to communication, socialization and activities of daily living.14 Social and economic consequences, including decreased ability to work and lifelong disability, may arise. This is even more profound in children having a recurrence. The financial impact of these consequences has yet to be analyzed.
CONCLUSION
AIS in the pediatric patient is a rare but potentially devastating disease. The lack of research in this area is apparent. There is only anecdotal evidence for the use of anti-thrombotic drugs in the management of children with ischemic strokes, unlike the evidence for treating adult ischemic strokes. Due to the high rate of recurrence anti-platelet drugs should be considered and initiated in the ED.
Footnotes
Chris Pastor, MD who provided this interesting case and patient followup.
Supervising Section Editor: Paul F. Walsh, MB, BCh, BAO, MSc
Submission history: Submitted March 22, 2008; Revision Received July 25, 2008; Accepted August 4, 2008.
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Julie Gorchynski, MD, MSc. 13546 Peseta Court, Corpus Christi, TX 78418
Email: jgorchyn@msn.com.
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Janjua N, et al. Thrombolysis for ischemic stroke in children: data from the nationwide inpatient sample. Stroke. 2007;38:1850–1854. [PubMed]
2. Nowak-Gottl, et al. Antithrombotic drug treatment of pediatric patients with ischemic stroke. Pediatric Drugs. 2003;5:167–175. [PubMed]
3. The International Stroke Trial (IST) A randomized trial of aspirin, subcutaneous heparin, both, or neither among 19435 patients with acute ischaemic stroke. International Stroke Trial Collaborative Group. Lancet. 1997;349:1569–1581. [PubMed]
4. National Institute of Neurological Disorders and Stroke rtPA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med. 1995;333:1581–1587.[PubMed]
5. Hacke W, et al. Intravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric stroke: the european cooperative acute stroke study.JAMA. 1995;274:1017–1025. [PubMed]
6. Multicentre Acute Stroke Trial Italy (MAST-I) Group. Randomised controlled trial of streptokinase, aspirin, and combination of both in treatment of acute ischaemic stroke.Lancet. 1995;346:1509–1514. [PubMed]
7. Williams GR. Incidence and characteristics of total stroke in the united states. BMC Neurol. 2001;1:2. [PMC free article] [PubMed]
8. Lee BI, et al. Yonsei Stroke Registry. Analysis of 1,000 patients with acute cerebral infarctions. Cerebrovasc Dis. 2001;12:145–151. [PubMed]
9. Lee Y, et al. Risk factors and outcomes of childhood ischemic stroke in taiwan. Brain and Development. 2007;30:14–19. [PubMed]
10. Fullerton HJ, Wu YW, Zhao S, Johnston SC. Risk of stroke in children: ethnic and gender disparities. Neurology. 2003;61:189–194. [PubMed]
11. Carpenter J, Tsuchida T, Lynch JK. Treatment of arterial ischemic stroke in children.Expert Review of Neurotherapeutics. 2007;7:383–394. [PubMed]
12. Shuayto MI, Lopez JI, Greiner F. Administration of intravenous tissue plasminogen activator in a pediatric patient with acute ischemic stroke. Journal of Child Neurology.2006;21:604–606. [PubMed]
13. Roach SE, et al. Management of Stroke in Infants and Children: A Scientific Statement From a Special Writing Group of the American Heart Association Stroke Council and the Council on Cardiovascular Disease in the Young. Stroke. 2008;39:2644–2691. [PubMed]
14. Hurvitz E, et al. Long-term functional outcome of pediatric stroke survivors. Topics in Stroke Rehabilitation. 2004;11:51–59. [PubMed]