{kind=link}

Brief Research Report
Treatment Protocol Assessment
Prospective Validation of Modified NEXUS Cervical Spine Injury Criteria in Low-risk Elderly Fall Patients
Westjem Read More
Emergency Department Access
Association of Insurance Status with Severity and Management in ED Patients with Asthma Exacerbation
Westjem Read More

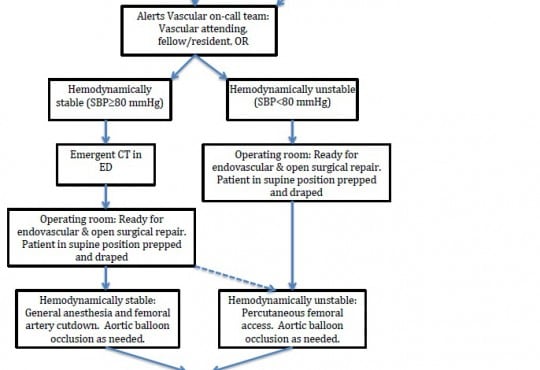
Treatment Protocol Assessment
Case Series of Patients with Ruptured Abdominal Aortic Aneurysm
Westjem Read More