
{kind=link}
| Author | Affiliation |
|---|---|
| Joseph Sinnott, MD | Washington University School of Medicine in St. Louis, Department of Emergency Medicine, St. Louis, Missouri |
| Christopher V. Holthaus, MD | Washington University School of Medicine in St. Louis, Department of Emergency Medicine, St. Louis, Missouri |
| Enyo Ablordeppey, MD, MPH | Washington University School of Medicine in St. Louis, Department of Emergency Medicine, St. Louis, Missouri; Washington University School of Medicine in St. Louis, Department of Anesthesiology, St. Louis, Missouri |
| Brian T. Wessman, MD | Washington University School of Medicine in St. Louis, Department of Emergency Medicine, St. Louis, Missouri; Washington University School of Medicine in St. Louis, Department of Anesthesiology, St. Louis, Missouri |
| Brian W. Roberts, MD, MSc | Cooper University Hospital, Department of Emergency Medicine, Camden, New Jersey |
| Brian M. Fuller, MD, MSCI | Washington University School of Medicine in St. Louis, Department of Emergency Medicine, St. Louis, Missouri; Washington University School of Medicine in St. Louis, Department of Anesthesiology, St. Louis, Missouri |
Introduction
Methods
Results
Discussion
Limitations
Conclusion
ABSTRACT
Introduction
Management of sedation, analgesia, and anxiolysis are cornerstone therapies in the emergency department (ED). Dexmedetomidine (DEX), a central alpha-2 agonist, is increasingly being used, and intensive care unit (ICU) data demonstrate improved outcomes in patients with respiratory failure. However, there is a lack of ED-based data. We therefore sought to: 1) characterize ED DEX use; 2) describe the incidence of adverse events; and 3) explore factors associated with adverse events among patients receiving DEX in the ED.
Methods
This was a single-center, retrospective, cohort study of consecutive ED patients administered DEX (January 1, 2017–July 1, 2019) at an academic, tertiary care ED with an annual census of ~90,000 patient visits. All included patients (n= 103) were analyzed for characterization of DEX use in the ED. The primary outcome was a composite of adverse events, bradycardia and hypotension. Secondary clinical outcomes included ventilator-, ICU-, and hospital-free days, and hospital mortality. To examine for variables associated with adverse events, we used a multivariable logistic regression model.
Results
We report on 103 patients. Dexmedetomidine was most commonly given for acute respiratory failure, including sedation for mechanical ventilation (28.9%) and facilitation of non-invasive ventilation (17.4%). Fifty-four (52.4%) patients experienced the composite adverse event, with hypotension occurring in 41 patients (39.8%) and bradycardia occurring in 18 patients (17.5%). Dexmedetomidine was stopped secondary to an adverse event in eight patients (7.8%). Duration of DEX use in the ED was associated with an increase adverse event risk (adjusted odds ratio, 1.004; 95% confidence interval, 1.001, 1.008).
Conclusion
Dexmedetomidine is most commonly administered in the ED for patients with acute respiratory failure. Adverse events are relatively common, yet DEX is discontinued comparatively infrequently due to adverse events. Our results suggest that DEX could be a viable option for analgesia, anxiolysis, and sedation in ED patients.
INTRODUCTION
The management of sedation, analgesia, and anxiolysis are critically important principles in the emergency department (ED). Dexmedetomidine (DEX) is a centrally acting and selective alpha-2 adrenoreceptor agonist, which inhibits norepinephrine release by binding to presynaptic alpha-2 receptors. It provides sedation, anxiolysis, and analgesia via receptors in the brainstem and spinal cord.1,2 Furthermore, DEX does not cause respiratory depression, making it an attractive agent for the management of multiple patient populations.
In patients with acute respiratory failure, data from mechanically ventilated intensive care unit (ICU) patients have demonstrated improved outcomes with DEX, when compared to benzodiazepines, including a reduction in delirium and ventilator duration.2-4 In ICU patients who cannot tolerate non-invasive positive pressure ventilation (NIPPV), DEX has been shown to be effective at facilitating NIPPV and may be associated with improved outcomes (ie, reduced intubation rates and ICU length of stay).1,5 However, there is a lack of data from the ED domain regarding DEX use in patients with acute respiratory failure. Other descriptions of DEX use in the ED include alcohol withdrawal and procedural sedation. Although the data are limited, a few studies have shown that DEX may reduce the need for endotracheal intubation in patients with alcohol withdrawal, and be a safe and effective procedural sedation agent.6-9
Given the lack of data and trials regarding DEX use in the ED, there is a significant knowledge gap and lack of familiarity regarding the use of this agent. Furthermore, as DEX has consistently been shown to increase the incidence of hypotension and bradycardia, its safety profile in the ED during routine use is unknown as well. We conducted this study with several objectives in mind: 1) to characterize the use of DEX in the ED; 2) describe the incidence of adverse events in the ED population; and 3) explore factors associated with adverse events among patients receiving DEX in the ED.
METHODS
Study Design
This was a single-center, retrospective, cohort study and is reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement (see supplemental Table S1). 10 The study was approved by the Human Research Protection Office at the principal investigator’s institution with waiver of informed consent. There was no financial support or funding organization associated with the study.
Study Setting and Population
The study was conducted at an academic, university-affiliated teaching hospital with an annual ED census of approximately 90,000 patient visits. Given the clinical outcome data regarding DEX, an order-set and protocol was introduced in the ED in 2017. This protocol advocated for a static DEX dose of 0.4 micrograms/kilogram/hour (mcg/kg/hour) in non-intubated patients. In mechanically ventilated patients, the protocol advocated for a starting dose of 0.7 mcg/kg/hour, with a recommended titration of 0.1 mcg/kg/hour every 45 minutes, up to a maximum dose of 1.5 mcg/kg/hour. Titration was by physician order, and not titratable by the nurse. Bolus doses of DEX were not recommended by the protocol, nor given during the study period. Over a 30-month period (January 1, 2017–July 1, 2019), all consecutive patients with an order to receive DEX were identified via electronic health record (EHR) query and were eligible for inclusion. Inclusion criteria were 1) age ≥ 18 years; and 2) the receipt of DEX in the ED for any indication.
Population Health Research Capsule
What do we already know about this issue?
Dexmedetomidine (DEX) provides sedation, anxiolysis, and analgesia and is effective in various clinical situations. However, data is sparse from the emergency department (ED) domain.
What was the research question?
How is DEX used in the ED, and what is the incidence of adverse events associated with its use?
What was the major finding of the study?
Dexmedetomidine is used primarily in respiratory failure (46.3% of cases). While adverse events are common (52.4% of cases), they are of questionable clinical significance.
How does this improve population health?
The use of dexmedetomidine could be an important adjunct in the care of multiple patient cohorts in the ED.
Study Protocol
Participant Selection and Data Collection
We identified patients with an order for DEX as receiving DEX in the ED by registry query, which was verified by review of the EHR. We excluded patients who did not actually receive DEX, as well as duplicate patients in the registry. All measurement and clinical data were gathered from the EHR using a standardized data collection form (created a priori), collated into an Excel 2016 (Microsoft Corporation, Redmond, WA, 2016) data management file, and exported to SPSS version 26, 2019 (IBM Corporation, Armonk, NY,) for management and data analysis. Prior to analysis, we checked the database for out-of-range and implausible values, and rechecked data as needed in the EHR to ensure accuracy. Baseline characteristics included the following: age; gender; race; body mass index; pre-existing comorbid conditions; disposition data; initial vital signs in the ED; and select laboratory values. Comorbid conditions were dementia, diabetes mellitus, cirrhosis, heart failure, end-stage renal disease, chronic obstructive pulmonary disease, immunosuppression, malignancy, alcohol abuse, and psychiatric illness (ie, schizophrenia, bipolar disorder, major depression, or generalized anxiety disorder). Laboratory values included lactate, creatinine, bilirubin, platelets, hemoglobin, and blood gases. The ED process of care variables included length of stay, vasopressor use, and need for mechanical ventilation.
We collected all DEX-related data in the ED including the following: indication for its use (per clinician documentation in the ED); time from ED arrival to order and time from order to drug administration; duration of use in the ED; dosing; and mental status (Richmond Agitation-Sedation Scale [RASS[ or Glasgow Coma Scale [GCS] at initiation. Additionally, we collected vital signs at initiation and their lowest values during drug infusion, and the number of patients in whom DEX was stopped in the ED, as well as co-administered analgesics and sedatives in the ED.
We collected details on adverse events and the treatment variables surrounding adverse events. The primary adverse events of interest included the incidence of hypotension and bradycardia. Similar to a prior large, randomized trial, hypotension was defined as a systolic blood pressure <80 millimeters mercury (mm Hg), a diastolic blood pressure <50 mm Hg, or > 30% decrease from baseline (systolic, diastolic, or mean arterial pressure). 3 Bradycardia was also defined based on prior trials, and included a heart rate < 40 beats per minute, < 60 beats per minute, or > 30% decrease from baseline.3,4 We also collected data regarding the need for vasoactive medications or fluid boluses after DEX initiation. If vasoactive medications or fluid boluses were given prior to DEX inititation, this was not counted as event secondary to DEX use. Finally, the cessation of DEX due to an adverse event was obtained from clinician documentation, and determined in the following manner: cessation due to hypotension and/or bradycardia, as defined in adverse events; or if cessation occurred due to inadvertent extubation.
An a priori subgroup of interest were the patients requiring mechanical ventilation in the ED.
Outcomes
We analyzed all included patients for characterization of DEX in the ED. The primary outcome of interest was the incidence of hypotension and bradycardia related to DEX use. Other clinical outcomes of interest included the incidence of acute brain dysfunction on ICU day 1 (delirium and coma), ventilator-, ICU- and hospital-free days, and hospital mortality. Coma was defined as having a RASS of −4 or −5 for every measurement while in the ICU. “Free” days account for both time (ie, duration of ventilation or lengths of stay) and mortality and are indexed to study day 28. In participants who survived 28 days, “-free” days are defined as 28 minus duration of ventilation (ventilator-free days) or length of stay (ICU- and hospital-free days). Participants who did not survive 28 days were assigned zero “-free” days.
Analysis
Patient characteristics are reported using descriptive statistics, including mean (standard deviation [SD]) and median (interquartile range [IQR]), and frequency distributions. We compared continuous variables using independent samples t-test or Mann-Whitney U test, whereas categorical variables were compared using chi-square test or Fisher’s exact test. We assessed the normality of the data by inspection of Q-Q plots and the Kolmogorov-Smirnov test.
For the purposes of this analysis, the primary outcome of adverse events was a composite outcome of hypotension or bradycardia. To examine for potential variables associated with adverse events we used a multivariable logistic regression model. In anticipation of a small number of events, we chose a parsimonious model and followed recommendations to select covariates a priori. 11 We therefore selected the following predictors for the model: 1) vasopressor infusion in the ED; 2) DEX duration in the ED; 3) heart rate at initiation of DEX; and 4) mechanical ventilation use in the ED. These variables were chosen for the following reasons: 1) Patients in shock may be more prone to experience hypotension related to DEX use; 2) a longer duration of use would allow greater time for adverse events to occur; 3) a lower baseline heart rate may lead to a higher incidence of bradycardia; and 4) mechanically ventilated patients are sicker and typically require more sedation than non-intubated patients, therefore predisposing them to a higher complication rate.
All tests were two-tailed with an alpha of 0.05 for statistical significance. As the study design is a retrospective cohort study over a fixed time frame, the sample size was limited to the number of patients receiving DEX during the course of routine care in the ED. Based on randomized trials examining DEX use in mechanically ventilated patients, we expected an adverse event rate ranging anywhere from 20–50%. 2-4 Assuming an estimated event (ie, composite adverse event) per covariable ratio of 10:1 necessary for multivariable logistic modeling, we assumed a sample size of 100 patients would be adequate to describe DEX use in the ED and explore factors associated with adverse events, in a hypothesis-generating multivariable model.12,13
RESULTS
A total of 103 patients were included in the study, and Figure 1 shows the study flow and final study population. Baseline characteristics are reported in Table 1. There was a statistical difference in peripheral oxygen saturation (mean [SD]) between patients experiencing an adverse event vs those who did not (93 [10] vs 96 [50], P = 0.018]. There were no other significant differences between patients experiencing an adverse event vs those who did not.
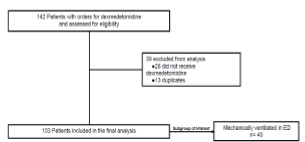
Table 1Characteristics of included study participants.
| Baseline characteristics | All subjects (n = 103) | No adverse event (n = 54) | Adverse event (n = 49) | P |
|---|---|---|---|---|
| Age (years) | 54 (37–65) | 55 (42–65) | 54 (35–65) | 0.692 |
| Female, n (%) | 39 (32.2) | 23 (42.6) | 16 (32.7) | 0.299 |
| BMI | 27.0 (22.4–35.0) | 29.1 (23.8–35.0) | 25.1 (21.1–35.8) | 0.248 |
| Race, n (%) | ||||
| Black | 52 (43.0) | 27 (50.0) | 25 (51.0) | 0.918 |
| White | 51 (42.1) | 27 (50.0) | 24 (49.0) | |
| Comorbidities, n (%) | ||||
| Dementia | 3 (2.5) | 1 (1.9) | 2 (4.1) | 0.502 |
| Diabetes mellitus | 31 (25.6) | 17 (31.5) | 14 (28.6) | 0.748 |
| Cirrhosis | 7 (5.8) | 4 (7.4) | 3 (6.1) | 0.796 |
| Heart failure | 16 (13.2) | 10 (18.5) | 6 (12.2) | 0.380 |
| ESRD | 5 (4.9) | 4 (7.4) | 1 (2.0) | 0.206 |
| COPD | 22 (18.2) | 14 (25.9) | 8 (16.3) | 0.235 |
| Alcohol abuse | 27 (22.3) | 16 (29.6) | 11 (22.4) | 0.408 |
| Illicit drug abuse | 29 (24.0) | 17 (31.5) | 12 (24.5) | 0.431 |
| Psychiatrica | 16 (13.2) | 6 (11.1) | 10 (20.4) | 0.193 |
| Disposition Data, n (%) | ||||
| Admit Location | 0.472 | |||
| ICU | 97 (80.2) | 50 (92.6) | 47 (95.9) | |
| Floor | 6 (5.0) | 4 (7.4) | 2 (4.1) | |
| Temperature (oC) | 36.7 (36.4–37.1) | 36.6 (36.3–37.0) | 36.7 (36.5–37.2) | 0.164 |
| Heart rate (bpm) | 107 (23) | 104 (23) | 109 (22) | 0.249 |
| Respiratory Rate (bpm) | 23 (7) | 23 (7) | 23 (7) | 0.684 |
| Systolic pressure (mm Hg) | 145 (30) | 143 (26) | 146 (33) | 0.646 |
| Diastolic pressure (mm Hg) | 89 (22) | 89 (21) | 88 (23) | 0.848 |
| Peripheral oxygen saturation (%) | 94 (8) | 96 (50) | 93 (10) | 0.018 |
| Lactate (mmol/L) | 2.3 (1.4–3.6) | 2.3 (1.4–3.5) | 2.2 (1.3–4.7) | 0.900 |
| Creatinine (mg/dL) | 1.0 (0.8–1.3) | 1.1 (0.8–1.3) | 1.0 (0.7–1.2) | 0.289 |
| Bilirubin (mg/dL) | 0.4 (0.3–0.6) | 0.4 (0.3–0.6) | 0.4 (0.3–0.8) | 0.616 |
| pH (n = 78) | 7.31 (0.13) | 7.31 (0.11) | 7.30 (0.14) | 0.560 |
| Partial pressure arterial oxygen (n=34) | 150 (76) | 144 (61) | 157 (93) | 0.628 |
| Partial pressure arterial or venous carbon dioxide (n = 78) | 48 (17) | 45 (11) | 52 (21) | 0.086 |
| SOFA score | 1.0 (0–4.0) | 1.0 (0–3.0) | 1.0 (1.0–4.0) | 0.697 |
| ED process of care variables | ||||
| Length of stay (hours) | 7.1 (4.7–9.6) | 6.7 (4.5–8.7) | 7.9 (5.2–10.3) | 0.101 |
| Vasopressor infusion, n (%) | 14 (11.6) | 4 (7.4) | 10 (20.4) | 0.055 |
| Mechanically ventilated, n (%) | 40 (33.1) | 24 (44.4) | 16 (32.7) | 0.220 |
aPsychiatric if diagnosed with schizophrenia, bipolar, major depression, or generalized anxiety disorder
Continuous variables are reported as mean (standard deviation) and median (interquartile range).
BMI, body mass index; ESRD, end-stage renal disease; COPD, chronic obstructive pulmonary disease; ICU, intensive care unit; C, Centigrade; bpm, beats per minute; bpm, breaths per minute; mm Hg, millimeters mercury; mmol/L, millimoles per liter; mg/dL, milligrams per deciliter; SOFA, sequential organ failure assessment; ED, emergency department.
Dexmedetomidine-related variables are shown in Table 2. Acute respiratory failure, including mechanical ventilation (28.9%) and NIPPV (17.4%), was the most common indication for DEX, followed by control of agitation (14.9%) and anxiety (11.6%). The median starting dose in the ED was 0.4 mcg/kg/hour (0.2 – 0.4). However, variability in starting dose did exist, as 16 patients were started at a dose of 0.7 mcg/kg/hour or higher (3 patients ≥ 1.0 mcg/kg/hour). Median infusion rate remained at 0.4 mcg/kg/hour for the first four hours, and the highest median infusion rate was 0.7 (0.4 – 0.9), demonstrating that, overall, relatively low doses of DEX were used in the ED. Dexmedetomidine was stopped in the ED in 22 (18.2%) patients. Co-administered analgesics and sedatives included fentanyl (39.8%); ketamine (36.9%); midazolam (33%); lorazepam (31.1%); haloperidol (28.2%); and propofol (27.2%).
Table 2Dexmedetomidine dosing and sedation characteristics.
| Variable | All subjects (n = 103) | No adverse event (n = 54) | Adverse event (n = 49) | P | ||||
|---|---|---|---|---|---|---|---|---|
| Indication for dexmedetomidine, n (%)* | 0.847 | |||||||
| Procedural sedation | 4 (3.3) | 2 (3.7) | 2 (4.1) | |||||
| Alcohol withdrawal | 9 (7.4) | 5 (9.3) | 4 (8.2) | |||||
| Anxiolysis | 14 (11.6) | 5 (9.3) | 9 (18.4) | |||||
| Psychosis/agitation | 18 (14.9) | 10 (18.5) | 8 (16.3) | |||||
| Facilitation of NIPPV | 21 (17.4) | 10 (18.5) | 11 (2.4) | |||||
| Sedation for mechanical ventilation | 35 (28.9) | 21 (38.9) | 14 (28.6) | |||||
| Other | 2 (1.7) | 1 (1.9) | 1 (2.0) | |||||
| Time from ED arrival to order (minutes) | 156 (64 – 317) | 170 (73 – 317) | 136 (42 – 333) | 0.722 | ||||
| Time from order to administration (minutes) | 26 (11 – 55) | 42 (16 – 60) | 21 (9 – 32) | 0.021 | ||||
| Duration of dexmedetomidine in ED (minutes) | 139 (74 – 211) | 122 (69 – 207) | 164 (96 – 240) | 0.041 | ||||
| Starting dose in ED (mcg/kg/hour) | 0.4 (0.2 – 0.4) | 0.4 (0.2 – 0.5) | 0.4 (0.2 – 0.4) | 0.267 | ||||
| RASS at initiation of dexmedetomidine (n= 29) | 1 (0 – 3) | 1 (−1 to 3) | 1 (0 – 2) | 0.811 | ||||
| GCS at initiation of dexmedetomidine (n= 40) | 13 (10 – 15) | 13 (11 – 15) | 13 (9 – 14) | 0.366 | ||||
| Co-administered analgesics and sedatives, n (%) | 0.248 | |||||||
| Fentanyl | 41 (39.8) | 23 (42.6) | 18 (36.7) | |||||
| Propofol | 28 (27.2) | 16 (29.6) | 12 (24.5) | |||||
| Midazolam | 34 (33.0) | 17 (31.5) | 17 (34.7) | |||||
| Ketamine | 38 (36.9) | 18 (33.3) | 20 (40.8) | |||||
| Lorazepam | 32 (31.1) | 15 (27.8) | 17 (34.7) | |||||
| Haloperidol | 25 (24.3) | 14 (25.9) | 11 (22.4) | |||||
| Vital signs | At initiation | Lowest during infusion | At Initiation | Lowest during infusion | At Initiation | Lowest during infusion | At initiation | Lowest during infusion |
| Heart rate (bpm) | 105 (23) | 86 (21) | 102 (21) | 91 (22) | 108 (25) | 81 (19) | 0.163 | 0.010 |
| Respiratory rate (bpm) | 23 (7) | 20 (18) | 24 (7) | 20 (6) | 23 (7) | 18 (5) | 0.697 | 0.051 |
| Systolic blood pressure (mm Hg) | 140 (29) | 112 (25) | 141 (27) | 124 (21) | 138 (32) | 99 (22) | 0.606 | <0.001 |
| Diastolic blood pressure (mm Hg) | 85 (24) | 68 (18) | 86 (20) | 77 (16) | 84 (27) | 58 (16) | 0.740 | <0.001 |
| Mean arterial pressure (mm Hg) | 101 (24) | 82 (19) | 102 (21) | 92 (16) | 100 (27) | 71 (16) | 0.796 | <0.001 |
| Dexmedetomidine infusion stopped in ED, n (%)a | 22 (18.2) | 11 (20.4) | 11 (22.4) | 0.797 | ||||
aEighteen patients were documented as having an additional secondary indication for dexmedetomidine use.
NIPPV, non-invasive positive pressure ventilation; ED, emergency department; mcg/kg/hour, micrograms/kilogram/hour; RASS, Richmond Agitation-Sedation Scale; GCS, Glasgow Coma Scale; bpm, beats per minute; bpm, breaths per minute; mm Hg, millimeters mercury.
Adverse events and clinical outcomes are reported in Table 3. Fifty-four (52.4%) patients experienced the composite adverse event, with hypotension occurring in 41 patients (39.8%) and bradycardia occurring in 18 patients (17.5%). Patients experiencing an adverse event were given a fluid bolus (20.4% vs 3.7%, P <0.01) and vasoactive medications (12.2% vs 3.7%, P = 0.11) more frequently when compared to patients without an adverse event. Dexmedetomidine was stopped secondary to an adverse event in eight patients (7.8%). Clinical outcomes for patients experiencing an adverse event vs those in patients with no adverse event (mean [SD]), were as follows: ventilator-free days, (20.4 [10.5] vs 22.6 [8.7], P = 0.44); ICU-free days, (21.7 [8.1] vs 21.3 [8.4], P = 0.83),; and hospital-free days (18.5 [8.1] vs 17.5 [8.7], P = 0.53). Mortality among patients experiencing an adverse event when compared to those with no adverse event was 10.2% vs 9.3%, P = 0.87.
Table 3Adverse events and clinical outcomes.
| Variable | All subjects (n = 103) |
|---|---|
| Hypotension, n (%) | 41 (39.8) |
| SBP <80 mm Hg | 8 (7.8) |
| DBP <50 mm Hg | 14 (13.6) |
| >30% decrease from baseline* | 19 (18.4) |
| Bradycardia, n (%)* | |
| <60 bpm | 18 (17.5) |
| <40 bpm | 0 (0.0) |
| Vasoactive medication given after dexmedetomidine initiated, n (%) | 8 (7.8) |
| Fluid bolus given after dexmedetomidine initiation, n (%) | 12 (11.7) |
| Cessation of dexmedetomidine due to adverse event, n (%) | 8 (7.8) |
| Starting dose in ED (mcg/kg/hour) | 0.4 (0.2 – 0.4) |
| Acute brain dysfunction on day 1 ICU, n (%) | |
| Delirium | 63 (61.2) |
| Coma | 0 |
| ICU-free days** | 21.5 (8.2) |
| Hospital-free days | 18.0 (8.4) |
| Hospital mortality, n (%) | 10 (9.7) |
*Refers to a decrease in systolic, diastolic, or mean arterial pressure.
**Refers to the 97 patients admitted to the intensive care unit from the emergency department.
Continuous variables are reported as mean (standard deviation) and median (interquartile range).
SBP, systolic blood pressure; DBP, diastolic blood pressure; bpm, beats per minute; ED, emergency department; mcg/kg/hour, micrograms/kilogram/hour; ICU, intensive care unit.
Table 4 shows the multivariable logistic regression analysis for predictors of the composite primary outcome. Duration of DEX use in the ED was associated with an increased risk for hypotension or bradycardia (adjusted odds ratio [aOR], 1.004; 95% CI, 1.001, 1.008), while vasopressor infusion in the ED was associated with a decrease risk (aOR, 0.21; 95% CI, 0.05, 0.82).
Table 4Multivariable logistic regression analysis with a composite of hypotension and bradycardia as the dependent variable.
| Variables | aOR | 95% CI | Standard error | P |
|---|---|---|---|---|
| Vasopressor infusion in the ED | 0.21 | 0.05 – 0.82 | 0.70 | 0.025 |
| Dexmedetomidine duration in the ED | 1.004 | 1.001 – 1.008 | 0.01 | 0.022 |
| Heart rate at initiation of dexmedetomidine | 1.01 | 0.99 – 1.03 | 0.01 | 0.238 |
| Mechanical ventilation in the ED | 1.63 | 0.60 – 4.40 | 0.51 | 0.341 |
ED, emergency department; aOR, adjusted odds ratio; CI, confidence interval.
Details regarding the mechanically ventilated subgroup are provided in supplemental tables S2–4. Overall, the dosing characteristics and adverse events experienced by mechanically ventilated patients were similar to the entire cohort.
DISCUSSION
As sedation and pain control are cornerstone therapies provided in the ED, and with the increase in use of DEX, information regarding its use in the ED is critical before quality improvement or future research can occur. The current study provides some new information regarding DEX use in the ED and builds on prior work by examining this agent in the ED domain.
With respect to our first objective, DEX is used for diverse indications in the ED, and most commonly for patients with respiratory failure. This is congruent with prior work and facilitated by DEX’s analgesic and sedative properties, without suppression of respiratory drive. The co-administration of other sedatives and analgesics was common, and could be driven by the known limitations of DEX, such as slower onset of action. There was a delay in administration of DEX (156 minutes) and relatively static dosing in the ED. This is likely driven by the lack of DEX in the ED (ie, ordered from pharmacy), as well as the institutional protocol, which called for no titration (in non-intubated patients) or physician-ordered titration (in mechanically ventilated patients). Going forward, areas for potential improvement could be as follows: 1) earlier identification of patients who may benefit from DEX, given the 2.5 hours of elapsed time from patient arrival to order; and 2) titrated dosing if DEX is tolerated, yet sedation goals have not been achieved.
Our most important finding relates to the adverse events experienced by ED patients given DEX. Prior work in difficult-to-sedate patients (n = 13) stated that DEX “is not safe in the ED setting.”14 Our results would suggest otherwise, and demonstrate that an ED-based DEX protocol can be effectively implemented. While adverse events were relatively common, the event rate for DEX use is congruent with that experienced in large randomized trials. 2-4 Also, when placed in the context of the reported incidence of hypotension with midazolam (11.6% to 55.7%) and propofol (13.4% to 52.4%) described in the literature, our results further suggest that DEX compares favorably in the ED setting.3,15,16 Furthermore, in only eight patients (7.8%) did physicians stop DEX due to an adverse event, suggesting that while hypotension and bradycardia were relatively common, these events were clinically well tolerated as judged by the treating team. Patients experiencing adverse events did require more intensive therapy in the ED, as demonstrated by the administration of more fluid boluses and vasoactive medications.
There was no statistical difference in patient-centered clinical outcomes between patients experiencing an adverse event when compared to those who did not. However, we urge caution in interpreting these clinical outcome data, given the small sample size. Contrary to our rationale for including vasopressors in the multivariable model, vasopressor infusion in the ED was associated with a lower chance for adverse events. It is possible that vasopressor titration reduced the risk of reported hypotension. While our study lacks granular detail on pressor requirements during DEX infusion, this finding is congruent with prior work showing that DEX is well tolerated in patients with shock. 17 A potentially important finding is the fact that duration of DEX exposure in the ED was associated with adverse events. While we lack specific detail on the exact timing of events, these data suggest the need for ongoing diligent monitoring for safety while DEX is being used in the ED.
Finally, in our subgroup of mechanically ventilated patients, the dosing of DEX and adverse events were comparable to non-intubated patients. While no definitive conclusions can be drawn from this small sample size, our findings suggest that DEX use in the ED could be a viable option going forward.
LIMITATIONS
This study has several limitations. This was a retrospective, single-center study that carries with it all of the limitations of that design, including limits with respect to generalizing these results to other centers, especially those where DEX use is infrequent in both the ED and ICU. While to our knowledge this is the largest ED-based DEX study to date, the small sample size limits any conclusions that can be drawn from these data. We further emphasize that point with respect to the subanalysis with an even smaller sample size and commensurate power limitations secondary to that. Due to an overall lack of sedation depth documentation, we cannot comment on the efficacy of DEX use in the ED. Future studies will need to assess for sedation depth, pain control, and anxiolysis in a much more granular fashion.
We defined our adverse events based on prior work from randomized trials on DEX in mechanically ventilated patients. While our adverse event rate was congruent with prior work, had our definition differed, the incidence of hypotension and bradycardia experienced in the ED could be lower than our current definition. This is especially important when considering that only eight patients had their DEX infusion stopped because of an adverse event. We also do not have details on why DEX was stopped outside of adverse events. It is possible that DEX was stopped because of inefficacy, or improving clinical trajectory. Due to the study design, it is impossible to ascribe causation for the adverse events, as multiple agents were used in addition to DEX, and we can only describe associations. Finally, due to the overall low event rate and small sample size, the results of our multivariable model should be considered exploratory and hypothesis-generating at this point.
CONCLUSION
Dexmedetomidine is most commonly administered in the ED for patients with acute respiratory failure (ie, those requiring mechanical ventilation or NIPPV). While adverse events are relatively common, they are of questionable clinical significance. Our results suggest that dexmedetomidine can be incorporated effectively into clinical care in the ED and be a viable option for analgesia, anxiolysis, and sedation in ED patients, similar to its role in the ICU.
Footnotes
Section Editor: Christopher Tainter, MD
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Brian M. Fuller, MD, MSCI, Washington University School of Medicine, Department of Emergency Medicine/Department of Anesthesiology, 660 S Euclid Avenue, St. Louis, Missouri 63110. Email: fullerb@wustl.edu. 9 / 2021; 22:1202 – 1209
Submission history: Revision received November 19, 2020; Submitted April 6, 2021; Accepted April 8, 2021
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. No author has professional or financial relationships with any companies that are relevant to this study. There are no conflicts of interest or sources of funding to declare.
REFERENCES
1. Huang Z, Chen Y-S, Yang Z-l, et al. Dexmedetomidine versus midazolam for the sedation of patients with non-invasive ventilation failure. Intern Med. 2012;51(17):2299-305.
2. Jakob S, Ruokonen E, Grounds RM, et al. Dexmedetomidine vs midazolam or propofol for sedation during prolonged mechanical ventilation: two randomized controlled trials. JAMA. 2012;307(11):1151-60.
3. Riker R, Shehabi Y, Bokesch P. SEDCOM (Safety and Efficacy of Dexmedetomidine Compared with Midazolam) Study Group Dexmedetomidine vs midazolam for sedation of critically ill patients: a randomized trial. JAMA. 2009;3015:489-99.
4. Pandharipande PP, Pun BT, Herr DL, et al. Effect of sedation with dexmedetomidine vs lorazepam on acute brain dysfunction in mechanically ventilated patients: the MENDS randomized controlled trial. JAMA. 2007;298(22):2644-53.
5. Senoglu N, Oksuz H, Dogan Z, et al. Sedation during noninvasive mechanical ventilation with dexmedetomidine or midazolam: a randomized, double-blind, prospective study. Curr Ther Res Clin Exp. 2010;71(3):141-53.
6. Long D, Long B, Koyfman A. The emergency medicine management of severe alcohol withdrawal. Am J Emerg Med. 2017;35(7):1005-11.
7. Godwin SA, Burton JH, Gerardo CJ, et al. Clinical policy: procedural sedation and analgesia in the emergency department. Ann Emerg Med. 2014;63(2):247-58.e18.
8. Jewett J, Phillips WJ. Dexmedetomidine for procedural sedation in the emergency department. Eur J Emerg Med. 2010;17(1):60.
9. Masoumi K, Maleki SJ, Forouzan A, et al. Dexmedetomidine versus midazolam-fentanyl in procedural analgesia sedation for reduction of anterior shoulder dislocation: a randomized clinical trial. Rev Recent Clin Trials. 2019;14(4):269-74.
10. von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Ann Intern Med. 2007;147(8):573-7.
11. Leisman DE, Harhay MO, Lederer DJ, et al. Development and reporting of prediction models: guidance for authors from editors of respiratory, sleep, and critical care journals. Crit Care Med. 2020;48(5):623.
12. Peduzzi P, Concato J, Feinstein AR, et al. Importance of events per independent variable in proportional hazards regression analysis II. Accuracy and precision of regression estimates. J Clin Epidemiol. 1995;48(12):1503-10.
13. Peduzzi P, Concato J, Kemper E, et al. A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol. 1996;49(12):1373-9.
14. Calver L, Isbister GK. Dexmedetomidine in the emergency department: assessing safety and effectiveness in difficult-to-sedate acute behavioural disturbance. Emerg Med J. 2012;29(11):915-8.
15. Jakob SM, Lubszky S, Friolet R, et al. Sedation and weaning from mechanical ventilation: effects of process optimization outside a clinical trial. J Crit Care. 2007;22(3):219-28.
16. Zhou Y, Jin X, Kang Y, et al. Midazolam and propofol used alone or sequentially for long-term sedation in critically ill, mechanically ventilated patients: a prospective, randomized study. Crit Care. 2014;18(3):1-9.
17. Morelli A, Sanfilippo F, Arnemann P, et al. The effect of propofol and dexmedetomidine sedation on norepinephrine requirements in septic shock patients: a crossover trial. Crit Care Med. 2019;47(2):e89-e95.