
{kind=link}
| Author | Affiliation |
|---|---|
| David Thompson, MD, MPH | Department of Emergency Medicine, Denver Health Medical Center, Denver, CO |
| Catherine Stanescu, MD | Department of Emergency Medicine, Denver Health Medical Center, Denver, CO |
| Peter Pryor, MD, MPH | Department of Emergency Medicine, Denver Health Medical Center, Denver, CO |
| Brooks Laselle, MD | Department of Emergency Medicine, Madigan Army Medical Center, Tacoma, WA |
ABSTRACT
The following case describes a 26-year-old female who presented to the emergency department with a nontrauamtic retrobulbar hematoma associated with warfarin toxicity. The application and limitations of focused bedside ocular sonography for this condition are discussed.
Video in axial plane of the left (symptomatic) orbit
[youtube=http://youtu.be/AWMladvbov0&w=500]Video in sagittal plane of the left (symptomatic) orbit
INTRODUCTION
Nontraumatic RBH occurs rarely and has been associated with arteriovenous malformations,1following thrombolysis,2 Type IV Ehlers-Danlos Syndrome,3 seizures,4 vomiting,5 following attempted strangulation, 5 and in a pregnant woman treated with subcutaneous heparin.6 To our knowledge this is the first case report of a RBH associated with warfarin toxicity.
CASE REPORT
A 26-year-old female presented to the emergency department (ED) with a chief complaint of left eye pain for the preceding three hours. After multiple episodes of emesis over 24 hours, the patient developed left eye pain and progressive swelling. She had a complicated medical history, including the recent diagnosis of deep venous thrombosis with associated pulmonary embolism 12 days prior, and initiation of warfarin therapy. Her past medical history included empyema, urosepsis, borderline personality disorder, pseudoseizures, chronic lymphadenopathy, peripheral neuropathy, and fibromyalgia.
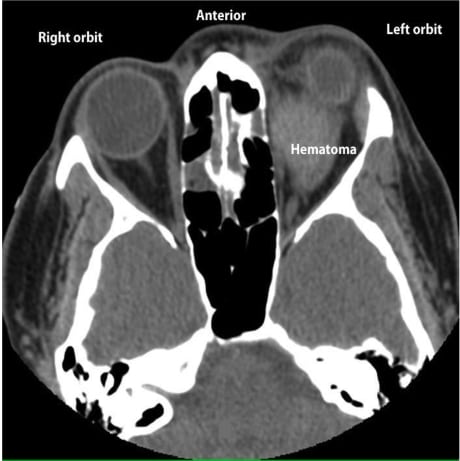
The physical exam was remarkable for slight left eye proptosis, left periorbital edema without evidence of trauma and an inferiorly displaced left gaze. Extraocular movements of the left eye were limited in attempted rightward gaze. Visual acuity seemed unchanged, as demonstrated by correct finger counting at four feet (the patient did not wear her contact lenses during the evaluation). Visual fields were intact. Intraocular pressure (IOP) was 30 mm Hg on the left, and 18mm Hg on the right. A focused bedside ocular ultrasound (Figure 1) was performed by an emergency ultrasound fellow. The ultrasound fellow had previously performed approximately 500 bedside ultrasound examinations and 15 ocular ultrasound evaluations. The findings of this examination were documented in real-time as: “compared to the asymptomatic eye there is evidence of slight proptosis and slight fullness of the soft-tissue in the retro-orbital region. There is no clear evidence of RBH, vitreous hemorrhage or retinal detachment.” Non-contrast head computed tomography (CT), obtained approximately 45 minutes after the bedside ultrasound, demonstrated a large left RBH with associated proptosis (Figure 2). No repeat ultrasound examination was performed following the head CT.

Following ophthalmology evaluation, the patient was admitted for reversal of her coagulopathy (INR 25) and observation. She subsequently developed worsening vision, an afferent papillary defect, and an increase in her IOP, which persisted following lateral canthotomy. She ultimately underwent a left orbitotomy for drainage of her RBH and relief of her orbital compartment syndrome.
DISCUSSION
We believe this is the first case report of a nontraumatic RBH associated with warfarin toxicity. Our patient also had vomiting, which may have been a causative factor.5 Similarly, nontraumatic RBH has been reported in other situations association with sudden elevation of cranial venous pressure and venous congestion (self-strangulation,7 induced by labor8 and scuba diving9), and systemic diseases associated with bleeding tendencies (coagulopathy from liver disease,10 scurvy11). In the elderly it has been postulated that vascular lesions, such as atherosclerosis or small aneurysms, could cause seemingly spontaneous hemorrhage, although a subacute presentation is more suggestive of venous bleeding. Occasionally, no associated etiology is found.
Without prompt recognition and treatment, RBH can lead to complications such as secondary optic atrophy, secondary strabismus, permanent choroidal folds, infection, hematoma enlargement and vision loss. Bedside ocular ultrasound is an appealing modality for rapid identification of this emergent condition and may obviate the need for CT scan if the diagnosis can be made.
In this case, the CT scan demonstrates a fairly significant RBH (Figure 2), yet the focused bedside ultrasound (Figure 1) failed to demonstrate a hypoechoic fluid collection in the retro-ocular region, as expected based on previous reports.12,13 Interestingly, in the emergency medicine literature no reports describe the sonographic diagnosis of RBH in a clinical setting. In 2000, Blaivas12 described the expected sonographic findings in a case series of ocular pathology identified with bedside ultrasound, although a specific case detailing the diagnosis of RBH was not reported. Also in 2000, an abstract published by Estevez et al.13 described accurate identification of simulated retrobulbar hematomas in bovine models with sonography, although the specific findings were not revealed. CT scan was used as a gold standard and the sonographers correctly identified 15/18 hematomas (83%) and 4/4 orbits without hematomas.
In this case, potential explanations for the paucity of findings on bedside ultrasound include: 1) incomplete evaluation of the retro-ocular region, 2) subsequent progression of the RBH following the ultrasound, 3) inexperience of the sonologist and 4) echogenicity incompatible with visualization of the RBH. These possibilities will be explored in further detail.
Incomplete ultrasound evaluation of the retro-ocular structures is possible considering the eccentric location of the RBH relative to the globe, as evidenced by CT (Figure 2). However, the sonologist spent approximately 15 minutes at the bedside performing a careful examination of the retro-orbital structures. Although the complete study was not recorded, two video clips were taken demonstrating interrogation of the symptomatic eye in both axial and sagittal planes [Videos 1, 2 (online at www.westjem.org)]. It should be noted that the sonologist feels these clips do not justify the full interrogation of the orbit actually performed at the time of the study. Regardless, an important point of emphasis is that a thorough ultrasound evaluation entails scanning all three dimensions of the structure(s) of interest.
Progression of the RBH in the brief period of time between the ultrasound evaluation and the CT is unlikely. It is clear that some progression of the RBH occurred during the hospital course. However, given the close proximity of the bedside ultrasound evaluation relative to the CT, and the fact that the patient’s condition remained unchanged during her stay in the ED, it is unlikely that significant change occurred during this time.
Inexperience of the sonologist for this technically challenging examination is worthy of consideration, although his reported comfort level with the examination was moderate to high.
Finally, echogenicity of the RBH may have played a factor. It is well known that acute blood often appears anechoic on ultrasound but over time becomes more echogenic. It seems likely, based on the onset of eye pain and swelling that the RBH occurred between a few hours and one day prior to presentation. This would suggest an isoechoic or hyperechoic RBH relative to the surrounding retro-ocular structures, composed of bone, fat and air (sinuses), all of which are echogenic structures. Yet, with such an extreme coagulopathy (INR = 25), this explanation is challenged.
The authors feel the most likely explanation for the false-negative ultrasound is similar echogenicity of the RBH and the surrounding retro-ocular tissues. Future investigations should explore the echogenicity of RBH of various ages (acute, subacute, chronic) and degrees of coagulopathy. Additional factors worth considering are the volume of blood necessary to produce a mass effect on the globe (notably this was not present in our patient), the ability to discern this finding on ultrasound, and correlation with patient symptoms.
Along with the expansion of bedside ultrasound in emergency departments worldwide, the applications of bedside ocular ultrasound are also increasing. For safe implementation, the strengths and limitations need to be elucidated. Although bedside ultrasound is helpful in the diagnosis of various ocular conditions in emergency medicine, further reports and/or studies are needed to determine the value for the diagnosis of RBH.14
CONCLUSION
In patients with proptosis and suspected retrobulbar hemorrhage, timely orbital decompression is essential to preserve the ocular nerve and visual acuity. While bedside ultrasound may be useful when positive, the diagnostic accuracy of this modality requires further investigation.
Footnotes
Supervising Section Editor: J Christian Fox MD, RDMS
Submission history: Submitted December 7, 2009; Revision Received March 20, 2010; Accepted March 29, 2010
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: David Thompson, MD, MPH, Department of Emergency Medicine, Denver Health Medical Center, 777 Bannock St., Denver, CO 80206
Email: davidothompson@gmail.com
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Moin M, Kersten RC, Bernardini F, et al. Spontaneous hemorrhage in an intraorbital arteriovenous malformation. Ophthalmology. 2000;107:2220–3. [PubMed]
2. Cunneen TS. Retro-orbital hemorrhage after thrombolysis for acute myocardial infarction. N Engl J Med. 2007;357:1448–9. [PubMed]
3. Shaikh S, Braun M, Eliason J. Spontaneous retrobulbar hemorrhage in type IV Ehlers-Danlos syndrome. Am J Ophthalmol. 2002;133:422–4. [PubMed]
4. Kue R. Retrobulbar hemorrhage resulting from syncopal seizures after a dental procedure. Am J Emerg Med. 2007;25:228–30. [PubMed]
5. Boyer M, Lucarelli M. Valsalva-Induced Subperiorbital Hemorrhage During Migraine. Arch Ophthalmol. 1998;116:106–7. [PubMed]
6. Chang WJ, Nowinski TS, Repke CS, Buerger DG. Spontaneous orbital hemorrhage in pregnant women treated with subcutaneous heparin. Am J Ophthalmol. 1996;122:907–8. [PubMed]
7. Knox Cartwright NE, Hussin HM, et al. Subperiosteal orbital hemorrhage following self-strangulation. Ann Ophthalmol. 2007;39:345–7.
8. Geyer O, Wasserman D, Rothkoff L, et al. Orbital haemorrhage induced by labour. Br J Ophthalmol.1990;74:242. [PMC free article] [PubMed]
9. Gómez-Ledesma I, Mencía-Gutíerrez E, et al. Subperiosteal Hemorrhage while Scuba Diving. Orbit.2006;25:19–22. [PubMed]
10. Moorthy RS, Yung CW, Nunery WR, et al. Spontaneous orbital subperiosteal hematoma of the orbit. Surg Neurol. 1983;20:100–2. [PubMed]
11. Sloan B, Kulwin DR, Kersten RC. Scurvy causing bilateralorbital hemorrhage. Arch Ophthalmol.1999;117:842–3. [PubMed]
12. Blaivas M. Bedside emergency department ultrasonography in the evaluation of ocular pathology. Acad Emerg Med. 2000;7:947–50. [PubMed]
13. Estevez A, Deutch J, Sturmann K, et al. Ultrasonography evaluation of retrobulbar hematoma in bovine orbits. Acad Emerg Med. 2000;7:1169–70. [PubMed]
14. Blaivas M, Theodoro D, Sierzenski P. A study of bedside ocular sonography in the emergency department. Acad Emerg Med. 2002;9:791–9. [PubMed]