On October 1, 2015, the United States Centers for Medicare and Medicaid Services (CMS) issued a core measure addressing the care of septic patients. These core measures are controversial among healthcare providers. This article will address that there is no gold standard definition for sepsis, severe sepsis or septic shock and the CMS-assigned definitions for severe sepsis and septic shock are premature and inconsistent with evidence-based definitions.
Administration of bolus intravenous (IV) antihypertensive treatment to lower BP in patients without a true hypertensive emergency is a wasteful practice that is discouraged by hypertension experts; however, anecdotal evidence suggests this occurs with relatively high frequency. Accordingly, we sought to assess the frequency of inappropriate IV antihypertensive treatment in ED patients with elevated BP absent a hypertensive emergency.
The electrocardiogram (ECG) is often used to identify which hyperkalemic patients are at risk for adverse events. However, there is a paucity of evidence to support this practice. This study analyzes the association between specific hyperkalemic ECG abnormalities and the development of short-term adverse events in patients with severe hyperkalemia.
Due to hospital crowding, mechanically ventilated patients are increasingly spending hours boarding in emergency departments (ED) before intensive care unit (ICU) admission. This study aims to evaluate the association between time ventilated in the ED and in-hospital mortality, duration of mechanical ventilation, ICU and hospital length of stay (LOS).
Endotracheal intubation (ETI) in the prehospital setting poses unique challenges where multiple ETI attempts are associated with adverse patient outcomes. Early identification of difficult ETI cases will allow providers to tailor airway-management efforts to minimize complications associated with ETI.
The California Prehospital Antifibrinolytic Therapy (Cal-PAT) study seeks to assess the safety and impact on patient mortality of tranexamic acid (TXA) administration in cases of trauma-induced hemorrhagic shock. The current study further aimed to assess the feasibility of prehospital TXA administration by paramedics within the framework of North American emergency medicine standards and protocols.
Necrotizing fasciitis (NF) is an uncommon but rapidly progressive infection that results in gross morbidity and mortality if not treated in its early stages. This study analyzed the ability of the LRINEC score to accurately rule out NF in patients who were confirmed to have cellulitis, as well as the capability to differentiate cellulitis from NF.
Our goal was to develop and validate an index to predict in-hospital mortality in older adults after non-traumatic emergency department (ED) intubations.
here is a subset of patients who suffer a witnessed ventricular fibrillation (VF) arrest and despite receiving reasonable care with medications (epinephrine and amiodarone) and multiple defibrillations (3+ attempts at 200 joules of biphasic current) remain in refractory VF (RVF), also known as electrical storm. The mortality for these patients is as high as 97%. We present the case of a patient who, with a novel approach, survived RVF to outpatient follow up.
The use of a noninvasive pelvic circumferential compression device (PCCD) to achieve pelvic stabilization by both decreasing pelvic volume and limiting inter-fragmentary motion has become commonplace, and is a well-established component of Advanced Trauma Life Support (ATLS) protocol in the treatment of pelvic ring injuries. The purpose of this study was to evaluate the following: 1) how consistently a PCCD was placed on patients who arrived at our hospital with unstable pelvic ring injuries; 2) if they were placed in a timely manner; and 3) if hemodynamic instability influenced their use.
Epinephrine is the treatment of choice for anaphylaxis. We surveyed emergency department (ED) healthcare providers regarding two methods of intramuscular (IM) epinephrine administration (autoinjector and manual injection) for the management of anaphylaxis and allergic reactions and identified provider perceptions and preferred method of medication delivery.
Resuscitation Prior to Emergency Endotracheal Intubation: Results of a National Survey
Robert S. Green, MD, et al.
Respiratory failure is a common problem in emergency medicine (EM) and critical care medicine (CCM). However, little is known about the resuscitation of critically ill patients prior to emergency endotracheal intubation (EETI). Our aim was to describe the resuscitation practices of EM and CCM physicians prior to EETI.
Volume 17, Issue 3, May 2016
Steve Christos, DO, MS et al.
Anticoagulation is the mainstay of medical treatment, prevention and reduction of recurrent venous thromboembolism, stroke prevention in patients with non-valvular atrial fibrillation, and it reduces the incidence of recurrent ischemic events and death in patients with acute coronary syndrome. Options for anticoagulation have been steadily increasing. Physicians need to be aware of the clinical profile of anticoagulation agents, reversal agents and treatment strategies in the face of major bleeding.
Volume 13, Issue 3, May 2016
Susan R. Wilcox, MD et al.
Introduction: Although emergency physicians frequently intubate patients, management of
mechanical ventilation has not been emphasized in emergency medicine (EM) education or clinical
practice. The objective of this study was to quantify EM attendings’ education, experience, and
knowledge regarding mechanical ventilation in the emergency department.
Methods: We developed a survey of academic EM attendings’ educational experiences with
ventilators and a knowledge assessment tool with nine clinical questions. EM attendings at key
teaching hospitals for seven EM residency training programs in the northeastern United States
were invited to participate in this survey study. We performed correlation and regression analyses
to evaluate the relationship between attendings’ scores on the assessment instrument and their
training, education, and comfort with ventilation.
Results: Of 394 EM attendings surveyed, 211 responded (53.6%). Of respondents, 74.5%
reported receiving three or fewer hours of ventilation-related education from EM sources over the
past year and 98 (46%) reported receiving between 0-1 hour of education. The overall correct
response rate for the assessment tool was 73.4%, with a standard deviation of 19.9. The factors
associated with a higher score were completion of an EM residency, prior emphasis on mechanical
ventilation during one’s own residency, working in a setting where an emergency physician bears
primary responsibility for ventilator management, and level of comfort with managing ventilated
patients. Physicians’ comfort was associated with the frequency of ventilator changes and EM
management of ventilation, as well as hours of education.
Conclusion: EM attendings report caring for mechanically ventilated patients frequently, but most
receive fewer than three educational hours a year on mechanical ventilation, and nearly half
receive 0-1 hour. Physicians’ performance on an assessment tool for mechanical ventilation is
most strongly correlated with their self-reported comfort with mechanical ventilation.
Volume 17, Issue 2, March 2016.
Justin Fulkerson, MSN, et al.
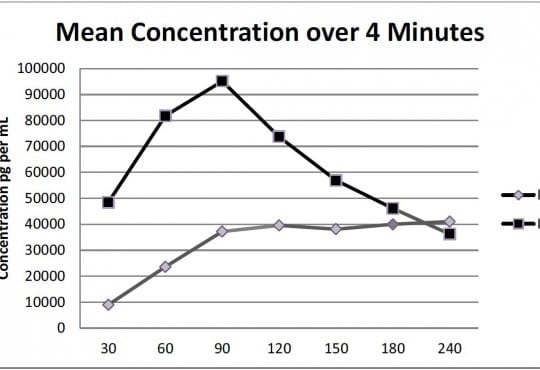
Introduction: This study compared the effects of vasopressin via tibial intraosseous (IO) and
intravenous (IV) routes on maximum plasma concentration (Cmax), the time to maximum
concentration (Tmax), return of spontaneous circulation (ROSC), and time to ROSC in a
hypovolemic cardiac arrest model.
Methods: This study was a randomized prospective, between-subjects experimental design. A
computer program randomly assigned 28 Yorkshire swine to one of four groups: IV (n=7), IO tibia
(n=7), cardiopulmonary resuscitation (CPR) + defibrillation (n=7), and a control group that received
just CPR (n=7). Ventricular fibrillation was induced, and subjects remained in arrest for two minutes.
CPR was initiated and 40 units of vasopressin were administered via IO or IV routes. Blood samples
were collected at 0.5, 1, 1.5, 2, 2.5, 3, and 4 minutes. CPR and defibrillation were initiated for
20 minutes or until ROSC was achieved. We measured vasopressin concentrations using highperformance
liquid chromatography.
Results: There was no significant difference between the IO and IV groups relative to achieving
ROSC (p=1.0) but a significant difference between the IV compared to the CPR+ defibrillation
group (p=0.031) and IV compared to the CPR-only group (p=0.001). There was a significant
difference between the IO group compared to the CPR+ defibrillation group (p=0.031) and IO
compared to the CPR-only group (p=0.001). There was no significant difference between the CPR
+ defibrillation group and the CPR group (p=0.127). There was no significant difference in Cmax
between the IO and IV groups (p=0.079). The mean ± standard deviation of Cmax of the IO group
was 58,709±25,463pg/mL compared to the IV group, which was 106,198±62,135pg/mL. There was
no significant difference in mean Tmax between the groups (p=0.084). There were no significant
differences in odds of ROSC between the tibial IO and IV groups.
Conclusion: Prompt access to the vascular system using the IO route can circumvent the
interruption in treatment observed with attempting conventional IV access. The IO route is an
effective modality for the treatment of hypovolemic cardiac arrest and may be considered first line for
rapid vascular access.
Volume 17, Issue 1, January 2016.
Adam J. Ash, DO, et al.
This is a case report describing the ultrasound-guided placement of a peripheral intravenous
catheter into the internal jugular vein of a patient with difficult vascular access. Although this
technique has been described in the past, this case is novel in that the Seldinger technique was
used to place the catheter. This allows for safer placement of a longer catheter (2.25”) without the
need for venous dilation, which is potentially hazardous.
Volume 16, Issue 7, December 2015.
Jarrod M. Mosier, MD, et al.
Airway management in critically ill patients involves the identification and management of the
potentially difficult airway in order to avoid untoward complications. This focus on difficult airway
management has traditionally referred to identifying anatomic characteristics of the patient that
make either visualizing the glottic opening or placement of the tracheal tube through the vocal
cords difficult. This paper will describe the physiologically difficult airway, in which physiologic
derangements of the patient increase the risk of cardiovascular collapse from airway management.
The four physiologically difficult airways described include hypoxemia, hypotension, severe
metabolic acidosis, and right ventricular failure. The emergency physician should account for
these physiologic derangements with airway management in critically ill patients regardless of the
predicted anatomic difficulty of the intubation.
Volume 16, Issue 7, December 2015.
Sundeep R. Bhat, MD
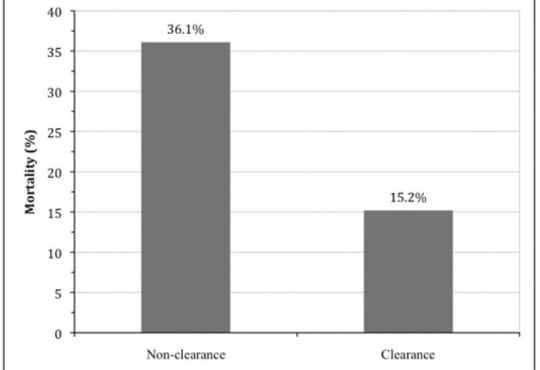
Introduction: Lactate clearance has been implicated as a predictor of mortality among emergency
department (ED) patients with severe sepsis or septic shock. We aimed to validate prior studies
showing that lactate clearance during the ED stay is associated with decreased mortality.
Methods: Retrospective dual-centered cross-sectional study using patients identified in the YaleNew
Haven Hospital Emergency Medicine sepsis registry with severe sepsis or septic shock who
had initial lactate levels measured in the ED and upon arrival (<24 hours) to the hospital floor.
Lactate clearance was calculated as percent of serum lactate change from ED to floor measurement.
We compared mortality and hospital interventions between patients who cleared lactate and those
who did not.
Results: 207 patients (110 male; 63.17±17.9 years) were included. Two reviewers extracted data
with 95% agreement. One hundred thirty-six patients (65.7%) had severe sepsis and 71 patients
(34.3%) had septic shock. There were 171 patients in the clearance group and 36 patients in the
non-clearance group. The 28-day mortality rates were 15.2% in the lactate clearance group and
36.1% in the non-clearance group (p<0.01). Vasopressor support was initiated more often in the nonclearance
group (61.1%) than in the clearance group (36.8%, p<0.01) and mechanical ventilation
was used in 66.7% of the non-clearance group and 36.3% of the clearance group (p=0.001).
Conclusion: Patients who do not clear their lactate in the ED have significantly higher mortality than
those with decreasing lactate levels. Our results are confirmatory of other literature supporting that
lactate clearance may be used to stratify mortality-risk among patients with severe sepsis or septic
shock.
Volume 16, Issue 7, December 2015.
Janice N. Thai, MD, et al.
Introduction: Penetrating injury to the forearm may cause an isolated radial or ulnar artery injury, or
a complex injury involving other structures including veins, tendons and nerves. The management of
forearm laceration with arterial injury involves both operative and nonoperative strategies. An evolution
in management has emerged especially at urban trauma centers, where the multidisciplinary resource
of trauma and hand subspecialties may invoke controversy pertaining to the optimal management of
such injuries. The objective of this review was to provide an evidence-based, systematic, operative
and nonoperative approach to the management of isolated and complex forearm lacerations. A
comprehensive search of MedLine, Cochrane Library, Embase and the National Guideline Clearinghouse
did not yield evidence-based management guidelines for forearm arterial laceration injury. No professional
or societal consensus guidelines or best practice guidelines exist to our knowledge.
Discussion: The optimal methods for achieving hemostasis are by a combination approach utilizing
direct digital pressure, temporary tourniquet pressure, compressive dressings followed by wound closure.
While surgical hemostasis may provide an expedited route for control of hemorrhage, this aggressive
approach is often not needed (with a few exceptions) to achieve hemostasis for most forearm lacerations.
Conservative methods mentioned above will attain the same result. Further, routine emergent or urgent
operative exploration of forearm laceration injuries are not warranted and not cost-beneficial. It has
been widely accepted with ample evidence in the literature that neither injury to forearm artery, nerve or
tendon requires immediate surgical repair. Attention should be directed instead to control of bleeding,
and perform a complete physical examination of the hand to document the presence or absence of other
associated injuries. Critical ischemia will require expeditious surgical restoration of arterial perfusion. In
a well-perfused hand, however, the presence of one intact artery is adequate to sustain viability without
long-term functional disability, provided the palmar arch circulation is intact. Early consultation with a hand
specialist should be pursued, and follow-up arrangement made for delayed primary repair in cases of
complex injury.
Conclusion: Management in accordance with well-established clinical principles will maximize treatment
efficacy and functional outcome while minimizing the cost of medical care.
Volume 16, Issue 7, December 2015.
Kelsey P. Mayrand, BS, et al.
Introduction: Current resuscitation guidelines emphasize a systems approach with a strong
emphasis on quality cardiopulmonary resuscitation (CPR). Despite the American Heart Association
(AHA) emphasis on quality CPR for over 10 years, resuscitation teams do not consistently meet
recommended CPR standards. The objective is to assess the impact on chest compression depth of
factors including bed height, step stool utilization, position of the rescuer’s arms and shoulders relative
to the point of chest compression, and rescuer characteristics including height, weight, and gender.
Methods: Fifty-six eligible subjects, including physician assistant students and first-year emergency
medicine residents, were enrolled and randomized to intervention (bed lowered and step stool
readily available) and control (bed raised and step stool accessible, but concealed) groups. We
instructed all subjects to complete all interventions on a high-fidelity mannequin per AHA guidelines.
Secondary end points included subject arm angle, height, weight group, and gender.
Results: Using an intention to treat analysis, the mean compression depths for the intervention
and control groups were not significantly different. Subjects positioning their arms at a 90-degree
angle relative to the sagittal plane of the mannequin’s chest achieved a mean compression
depth significantly greater than those compressing at an angle less than 90 degrees. There was
a significant correlation between using a step stool and achieving the correct shoulder position.
Subject height, weight group, and gender were all independently associated with compression depth.
Conclusion: Rescuer arm position relative to the patient’s chest and step stool utilization during
CPR are modifiable factors facilitating improved chest compression depth.
Volume 16, Issue 5, September 2015.
Christian D. McClung, MD, MPhil, et al.
Interposed abdominal compression cardiopulmonary resuscitation (IAC-CPR) is an alternative
technique to traditional cardiopulmonary resuscitation (CPR) that can improve perfusion and lead to
restoration of circulation in patients with chest wall deformity either acquired through vigorous CPR
or co-morbidity such as chronic obstructive pulmonary disease. We report a case of out-of-hospital
cardiac arrest where IAC-CPR allowed for restoration of spontaneous circulation and eventual
full neurologic recovery when traditional CPR was failing to generate adequate pulses with chest
compression alone.
Volume 16, Issue 4, July 2015
Kevin Lu, BS, et al.
Missile embolization is regarded as a rare phenomenon in the world of penetrating trauma. While figures in the world of civilian trauma do not exist, there is reason to believe that missile emboli are frequent enough to warrant the attention of any medical decision maker who cares for trauma patients.
Volume 16, Issue 3, May 2015
Daniel Aronovich, DO, et al.
There has been an increase in patients having serum lactate drawn in emergency situations. The objective of this study was to determine whether or not it was necessary to obtain a lactate level in patients with a normal serum bicarbonate level and anion gap. This is a retrospective chart review evaluation of 304 patients who had serum lactate and electrolytes measured in an emergency setting in one academic medical center.
Volume 16, Issue 1, January 2015
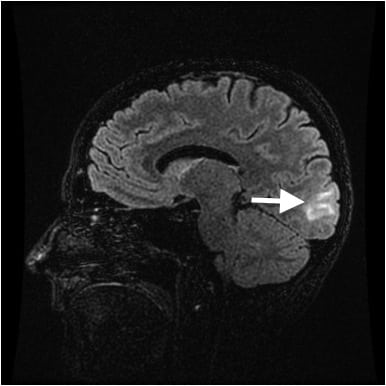
Ryan J. Thompson, MD et al.
Posterior Reversible Encephalopathy Syndrome (PRES) often has variable presentations and causes, with common radiographic features—namely posterior white matter changes on magnetic resonance (MRI). As MRI becomes a more frequently utilized imaging modality in the Emergency Department, PRES will become an entity that the Emergency Physician must be aware of and be able to diagnose.
Volume 15, Issue 7, November 2014
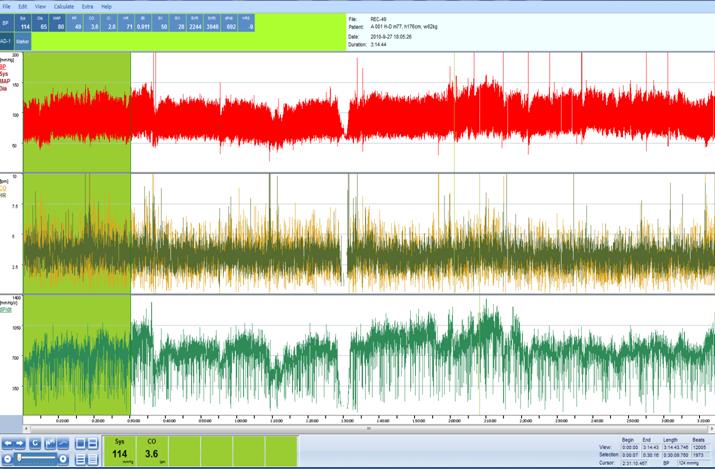
Richard M. Nowak, MD et al.
Noninvasive hemodynamic (HD) assessments in the emergency department (ED) might assist in the diagnosis, therapeutic plan development and risk stratification of acutely ill patients.
Volume 15, Issue 7, November 2015
Edward P. Sloan, MD, MPH et al.
To assess the ability of the shock index (SI) to predict 28-day mortality in traumatic hemorrhagic shock patients treated in the diaspirin cross-linked hemoglobin (DCLHb) resuscitation clinical trials.
{kind=link}