Patient navigation programs can help people overcome barriers to outpatient care. Patient experiences with these programs are not well understood. The goal of this study was to understand patient experiences and satisfaction with an emergency department (ED)-initiated patient navigation (ED-PN) intervention for US Medicaid-enrolled frequent ED users.
Many medical students and residents feel stressed and uncomfortable with such situations because of insufficient training. Our randomized controlled study aimed to assess the efficacy of a four-hour BBN simulation-based training on perceived self-efficacy, the BBN process, and communication skills.
The goals of this study were to determine whether Press Ganey ED satisfaction scores for emergency physicians working at two different sites were consistent between sites, and to identify factors contributing to any variation.
Our study compared the medical histories obtained by physicians in the emergency department (ED) based on whether the patients primarily spoke English or Spanish.
Volume 17, Issue 4, July 2016
C. Ferrell Varner, MD
Below is a letter concerning contact with patients. I have found this practice useful. It decreases anxiety on the part of the patient and the doctor. I write to recommend it to emergency physicians everywhere.
I give my cell phone number to patients all the time. By that I mean 2–3 times a shift. I have been doing it for years, almost since I first got a cell phone. I have given it out hundreds of times. I recommend that we encourage our emergency medicine (EM) residents to do so also. It is an easy option, and it can help avoid all sorts of problems. Discretion is in order, but there are not a lot of exceptions. There are some types of patients that I do not give it to.
Volume 16, Issue 7, December 2015.
Daniel J. Henning, MD, MPH, et al.
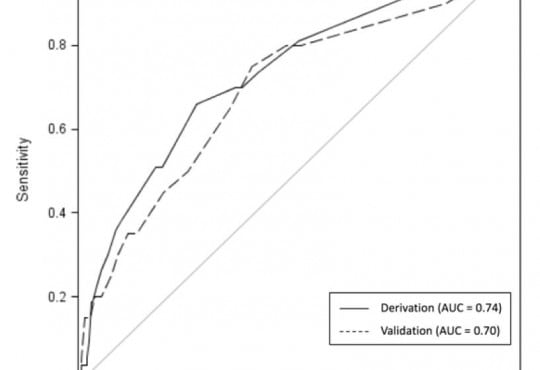
Introduction: Strategies to identify high-risk emergency department (ED) patients often use markedly
abnormal vital signs and serum lactate levels. Risk stratifying such patients without using the presence of
shock is challenging. The objective of the study is to identify independent predictors of in-hospital adverse
outcomes in ED patients with abnormal vital signs or lactate levels, but who are not in shock.
Methods: We performed a prospective observational study of patients with abnormal vital signs or lactate
level defined as heart rate ≥130 beats/min, respiratory rate ≥24 breaths/min, shock index ≥1, systolic
blood pressure <90mm/Hg, or lactate ≥4mmole/L. We excluded patients with isolated atrial tachycardia,
seizure, intoxication, psychiatric agitation, or tachycardia due to pain (ie: extremity fracture). The primary
outcome was deterioration, defined as development of acute renal failure (creatinine 2x baseline), nonelective
intubation, vasopressor requirement, or mortality. Independent predictors of deterioration after
hospitalization were determined using logistic regression.
Results: Of 1,152 consecutive patients identified with abnormal vital signs or lactate level, 620 were
excluded, leaving 532 for analysis. Of these, 53/532 (9.9±2.5%) deteriorated after hospital admission.
Independent predictors of in-hospital deterioration were: lactate >4.0mmol/L (OR 5.1, 95% CI [2.1–12.2]),
age ≥80 yrs (OR 1.9, CI [1.0–3.7]), bicarbonate <21mEq/L (OR 2.5, CI [1.3–4.9]), and initial HR≥130 (OR
3.1, CI [1.5–6.1]).
Conclusion: Patients exhibiting abnormal vital signs or elevated lactate levels without shock had
significant rates of deterioration after hospitalization. ED clinical data predicted patients who suffered
adverse outcomes with reasonable reliability.
Volume 16, Issue 7, December 2015.
Matthew C. DeLaney, MD, et al.
Introduction: Patient satisfaction is a commonly assessed dimension of emergency department (ED)
care quality. The ability of ED clinicians to estimate patient satisfaction is unknown. We sought to
evaluate the ability of emergency medicine resident physicians and nurses to predict patient-reported
satisfaction with physician and nursing care, pain levels, and understanding of discharge instructions.
Methods: We studied a convenience sample of 100 patients treated at an urban academic ED.
Patients rated satisfaction with nursing care, physician care, pain level at time of disposition and
understanding of discharge instructions. Resident physicians and nurses estimated responses
for each patient. We compared patient, physician and nursing responses using Cohen’s kappa,
weighting the estimates to account for the ordinal responses.
Results: Overall, patients had a high degree of satisfaction with care provided by the nurses and
physicians, although this was underestimated by providers. There was poor agreement between
physician estimation of patient satisfaction (weighted κ=0.23, standard error: 0.078) and nursing
estimates of patient satisfaction (weighted κ=0.11, standard error: 0.043); physician estimation
of patient pain (weighted κ=0.43, standard error: 0.082) and nursing estimates (weighted κ=0.39,
standard error: 0.081); physician estimates of patient comprehension of discharge instruction
(weighted κ=0.19, standard error: 0.082) and nursing estimates (weighted κ=0.13, standard error:
0.078). Providers underestimated pain and patient comprehension of discharge instructions.
Conclusion: ED providers were not able to predict patient satisfaction with nurse or physician
care, pain level, or understanding of discharge instructions.
Volume 16, Issue 7, December 2015.
Ramsey C. Tate, MD, MS
Introduction: Despite evidence from other healthcare settings that language barriers negatively
impact patient outcomes, the literature on language barriers in emergency medical services (EMS)
has not been previously summarized. The objective of this study is to systematically review existing
studies of the impact of language barriers on prehospital emergency care and identify opportunities
for future research.
Methods: A systematic review with narrative synthesis of publications with populations specific to
the prehospital setting and outcome measures specific to language barriers was conducted. A fourprong
search strategy of academic databases (PubMed, Academic Search Complete, and Clinical
Key) through March 2015, web-based search for gray literature, search of citation lists, and review
of key conference proceedings using pre-defined eligibility criteria was used. Language-related
outcomes were categorized and reported as community-specific outcomes, EMS provider-specific
outcomes, patient-specific outcomes, or health system-specific outcomes.
Results: Twenty-two studies met eligibility criteria for review. Ten publications (45%) focused on
community-specific outcomes. Language barriers are perceived as a barrier by minority language
speaking communities to activating EMS. Eleven publications (50%) reported outcomes specific
to EMS providers, with six of these studies focused on EMS dispatch. EMS dispatchers describe
less accurate and delayed dispatch of resources when confronted with language discordant callers,
as well as limitations in the ability to provide medical direction to callers. There is a paucity of
research on EMS treatment and transport decisions, and no studies provided patient-specific or
health system-specific outcomes. Key research gaps include identifying the mechanisms by which
language barriers impact care, the effect of language barriers on EMS utilization and clinically
significant outcomes, and the cost implications of addressing language barriers.
Conclusion: The existing research on prehospital language barriers is largely exploratory, and
substantial gaps in understanding the interaction between language barriers and prehospital care
have yet to be addressed. Future research should be focused on clarifying the clinical and cost
implications of prehospital language barriers.
Volume 16, Issue 7, December 2015.
Kory S. London, MD, et al.
Introduction: Feedback on patient satisfaction (PS) as a means to monitor and improve
performance in patient communication is lacking in residency training. A physician’s promotion,
compensation and job satisfaction may be impacted by his individual PS scores, once he is in
practice. Many communication and satisfaction surveys exist but none focus on the emergency
department setting for educational purposes. The goal of this project was to create an emergency
medicine-based educational PS survey with strong evidence for content validity.
Methods: We used the Delphi Method (DM) to obtain expert opinion via an iterative process of
surveying. Questions were mined from four PS surveys as well as from group suggestion. The DM
analysis determined the structure, content and appropriate use of the tool. The group used four-point
Likert-type scales and Lynn’s criteria for content validity to determine relevant questions from the
stated goals.
Results: Twelve recruited experts participated in a series of seven surveys to achieve consensus. A
10-question, single-page survey with an additional page of qualitative questions and demographic
questions was selected. Thirty one questions were judged to be relevant from an original 48-question list.
Of these, the final 10 questions were chosen. Response rates for individual survey items was 99.5%.
Conclusion: The DM produced a consensus survey with content validity evidence. Future work will
be needed to obtain evidence for response process, internal structure and construct validity.
Volume 16, Issue 5, September 2015.
Clayton Wu, MD, et al.
Introduction: Understanding patient perceptions and preferences of hospital care is important to
improve patients’ hospitalization experiences and satisfaction. The objective of this study was to
investigate patient preferences and perceptions of hospital care, specifically differences between
intensive care unit (ICU) and hospital floor admissions.
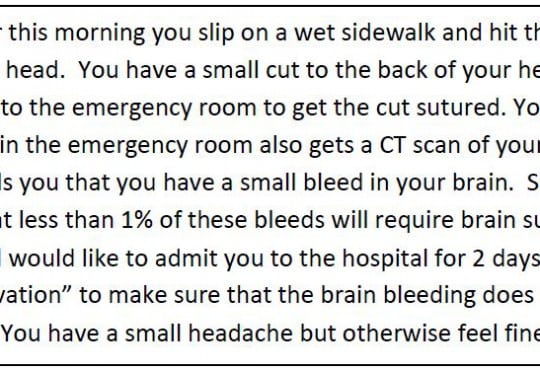
Methods: This was a cross-sectional survey of emergency department (ED) patients who were
presented with a hypothetical scenario of a patient with mild traumatic brain injury (TBI). We
surveyed their preferences and perceptions of hospital care related to this scenario. A closed-ended
questionnaire provided quantitative data on patient preferences and perceptions of hospital care and
an open-ended questionnaire evaluated factors that may not have been captured with the closedended
questionnaire.
Results: Out of 302 study patients, the ability for family and friends to visit (83%), nurse availability
(80%), and physician availability (79%) were the factors most commonly rated “very important,” while
the cost of hospitalization (62%) and length of hospitalization (59%) were the factors least commonly
rated “very important.” When asked to choose between the ICU and the floor if they were the patient
in the scenario, 33 patients (10.9%) choose the ICU, 133 chose the floor (44.0%), and 136 (45.0%)
had no preference.
Conclusion: Based on a hypothetical scenario of mild TBI, the majority of patients preferred
admission to the floor or had no preference compared to admission to the ICU. Humanistic factors
such as the availability of doctors and nurses and the ability to interact with family appear to have a
greater priority than systematic factors of hospitalization, such as length and cost of hospitalization
or length of time in the ED waiting for an in-patient bed.
{kind=link}