
{kind=link}
| Author | Affiliation |
|---|---|
| Monica H Swahn, PhD, MPH | Georgia State University, Institute of Public Health, Atlanta, Georgia |
| Lindsay Gressard, M. Ed., MPH | Georgia State University, Institute of Public Health, Atlanta, Georgia |
| Jane B Palmier, J.D., MPH | Georgia State University, Institute of Public Health, Atlanta, Georgia |
| Rogers Kasirye, M.A | Uganda Youth Development Link, Kampala, Uganda |
| Catherine Lynch, MD | Duke University, Department of Surgery and Emergency Medicine, Durham, North Carolina |
| Huang Yao, M.A | Georgia State University, Institute of Public Health, Atlanta, Georgia |
ABSTRACT
Introduction:
Violence among youth is a major public health issue globally. Despite these concerns, youth violence surveillance and prevention research are either scarce or non-existent, particularly in developing regions, such as sub-Saharan Africa. The purpose of this study is to quantitatively determine the prevalence of violence involving weapons in a convenience sample of service-seeking youth in Kampala. Moreover, the study will seek to determine the overlap between violence victimization and perpetration among these youth and the potentially shared risk factors for these experiences.
Methods:
We conducted this study of youth in May and June of 2011 to quantify and describe high-risk behaviors and exposures in a convenience sample (N=457) of urban youth, 14–24 years of age, living on the streets or in the slums and who were participating in a Uganda Youth Development Link drop-in center for disadvantaged street youth. We computed bivariate and multivariate logistic regression analyses to determine associations between psychosocial factors and violence victimization and perpetration.
Results:
The overall prevalence of reporting violence victimization involving a weapon was 36%, and violence perpetration with a weapon was 19%. In terms of the overlap between victimization and perpetration, 16.6% of youth (11.6% of boys and 24.1% of girls) reported both. In multivariate analyses, parental neglect due to alcohol use (Adj.OR=2.28;95%CI: 1.12—4.62) and sadness (Adj.OR=4.36 ;95%CI: 1.81—10.53) were the statistically significant correlates of victimization only. Reporting hunger (Adj.OR=2.87 ;95%CI:1.30—6.33), any drunkenness (Adj.OR=2.35 ;95%CI:1.12—4.92) and any drug use (Adj.OR=3.02 ;95%CI:1.16—7.82) were significantly associated with both perpetration and victimization.
Conclusion:
The findings underscore the differential experiences associated with victimization and perpetration of violence involving weapons among these vulnerable youth. In particular, reporting hunger, drunkenness and drug use were specifically associated with victimization and perpetration. These are all modifiable risk factors that can be prevented. It is clear that these vulnerable youth are in need of additional services and guidance to ameliorate their adverse childhood experiences, current health risk behaviors and disadvantaged living context.
INTRODUCTION
Violence is a major global public health problem.1 However, the concern is primarily for adolescents and young adults who are typically the primary perpetrators and victims of interpersonal violence.2Unfortunately, youth violence surveillance and prevention research are either scarce or non-existent in many countries, particularly in low- and middle-income regions, such as Africa and South America.1,3Limited existing data suggest that these areas are those in which youth homicide rates are the highest.2,4 Moreover, rapid urbanization, economic instability, and civil unrest are recognized as particularly salient risk factors for violence. 2
In sub-Saharan Africa, political and economic stability remain distant goals as the HIV/AIDS epidemic continues to disproportionately devastate the 15–24 year-old population, leaving the region without its most productive citizens, which significantly impacts its prosperity. 5–6 Estimates also indicate a growing population of orphans and unfortunately, orphans typically experience a range of adverse outcomes.7–9 Due to the limited economic security and regional stability, youth violence is likely to remain a substantial problem in this region. Research of the relatively few data sources available also indicate that school-attending youth in five different sub-Saharan countries report relatively high levels of youth violence.3,10
Violence among children and adolescents living on the streets or in the slums of sub-Saharan Africa is of particular concern. Commonly referred to as “street children,” these youth are typified by living or earning income on the streets and by a lack of adequate adult supervision. Although the extent to, and the reasons for, which these youth live on the streets varies, economic hardship, family conflict or disruption, and abuse or maltreatment are often predisposing situational factors.9,11–13 Because girls are more frequently engaged in domestic work in developing countries, boys account for a disproportionate number of street children.9,11,13
The lives of street children are often marked by poverty, family conflict, low parental attachment, as well as alcohol and drug use, which are factors that have been established to increase risk for interpersonal violence.2,14 Furthermore, street children are often viewed collectively as a societal nuisance and are consequently subjected to varying degrees of abuse and violence from police officers, retail business owners, and other community members.9,15 For some street children, the effects of this physical brutality may compound the mental and emotional scars caused by the parental abuse that may have precipitated their living on the streets.11,15 Exposure to violence such as this has been shown to increase the risk for becoming a perpetrator of violence in the future.16 Moreover, other risk factors for violence include experiencing hunger, substance use, low academic achievement, poor school attendance, health problems, and having delinquent peers.2,16,17
The purpose of this study was to quantitatively determine the prevalence of violence involving weapons among a convenience sample of service-seeking youth who live in the slums of Kampala, the capital city of Uganda. Moreover, the study sought to determine the co-occurrence or overlap between violence victimization and perpetration among these youth and the potentially shared risk factors for these experiences. Recent research has called for violence prevention research to more specifically examine the perpetration and victimization of violence in order to provide additional context for prevention strategies.19,20 Understanding the needs of street children in Uganda is particularly crucial because Uganda is expected to have the world’s highest rate of population growth in coming years.21Furthermore, recent years of civil unrest and violence make Uganda’s street children especially susceptible.22 Therefore, the results of this study may be used to provide guidance on the development of prevention strategies to address the violence experiences this vulnerable population faces.
METHODS
Survey Participants and Recruitment
The overarching goal of the cross-sectional survey called the “Kampala Youth Survey,” conducted in May and June 2011, was to quantify and describe high-risk behaviors and exposures in a convenience sample of urban youth (14 to 24 years of age) living on the streets or in the slums and who were participating in a Uganda Youth Development Link (UYDEL) drop-in center for disadvantaged street youth. 23 UYDEL is a not for profit organization that operates eight centers with a primary goal of reducing risk behaviors such as HIV acquisition and drug use. They typically serve about 650 youth per month through these drop-in centers. Face-to-face surveys, lasting approximately 30 minutes, were administered by social workers/peer educators employed by UYDEL to ensure valid survey administration and to assist with any language barriers. The study was implemented across eight drop-in centers throughout Kampala. Participating youth received snacks and transportation for completing the survey. No identifying information was collected and the surveys were completely anonymous. Surveys were administered in English or Uganda’s local language Luganda, and to the extent possible, in private locations, to ensure privacy of survey questions and responses.
Each social worker/peer educator received training on the study methodology, all survey items, and, if needed, how to verbally translate the consent forms and survey questions into Luganda. After training, they initiated the recruitment of potential participants among attendants at their specific drop-in center. Recruitment took place using word-of-mouth, and each attendant was eligible for participation if they were between 14 and 24 years of age. No other exclusion criteria were used. Participants were informed about the study and read (or were read) the consent forms to indicate their willingness to take the survey. In Uganda, youth 14 to 17 years of age, who “cater for their own livelihood” are considered emancipated and are able to provide their own consent for participating in the survey. The same consent process was followed for youth 18 to 24 years of age.
Over the 10-day survey period, 507 youth were approached and asked to participate in the survey. Among these youth, 46 declined and 461 agreed to participate, yielding a participation rate of 90.9%. Four of the surveys were missing substantial numbers of responses and were therefore excluded, yielding 457 completed surveys for the final analytic sample of youth between the ages of 14 and 24 (31.1% boys and 68.5% girls). The mode for age was 17 years (n=81) and 67% of participants were between ages 16 and 20.
Survey Measures
The survey questionnaire was modeled from existing surveys such as the Youth Risk Behavior Survey24conducted by the Centers for Disease Control and Prevention (CDC) in the U.S. and the international Global School-based Student Health Survey25 supported by the World Health Organization. Survey questions addressed demographic characteristics, family context, alcohol and drug use, injuries, violence and suicidal behaviors, sexual behaviors and sexually transmitted diseases, including HIV/AIDS.
Ethical Approvals
The study protocol was approved by the Georgia State University Institutional Review Board and by the Uganda National Council for Science and Technology. Funding to conduct the study was obtained from the Georgia State University International Strategic Initiative and also from funds leveraged through collaboration with the Emory Center for Injury Control, funded by the CDC.
Data Analysis
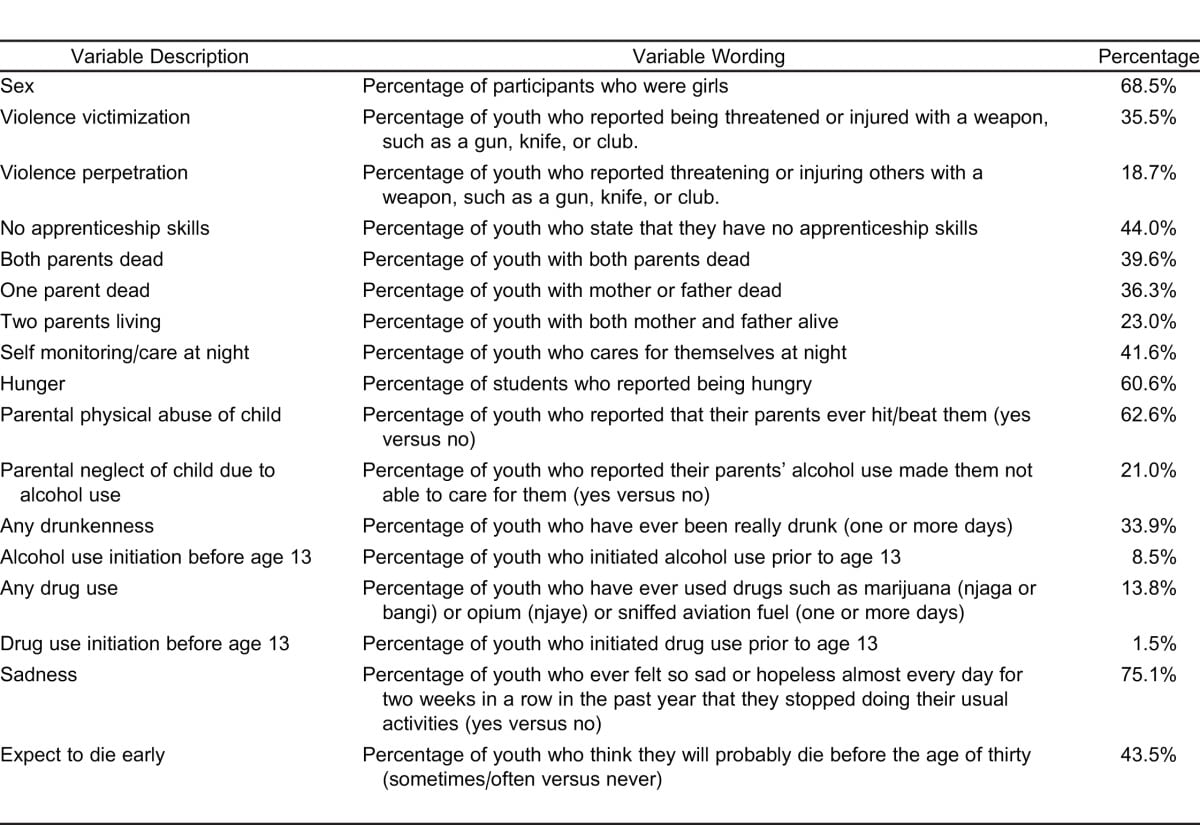
The measures included in the analyses and their prevalence among study participants are described in Table 1 and were selected based on previous theoretical and empirical research indicating their potential importance in violence victimization and perpetration.2,10,14,17 We created the outcome variable by combining the measures on violence victimization and perpetration, yielding 4 mutually exclusive categories: 1) No violence; 2) Perpetration only; 3) Victimization only; and 4) Both perpetration and victimization.
We computed bivariate and multivariate multilogistic regression analyses to determine the statistical associations between demographic and psychosocial correlates and violence victimization and perpetration using the SAS 9.2 (SAS institute) and SUDAAN 10 (RTI) (statistical software packages). We dichotomized most variables to indicate the presence or absence of the particular risk factor. The reference category for each variable in the logistic regression analyses was the absence of the particular risk factor.
RESULTS
The demographic characteristics and psychosocial characteristics, as well as prior experience with child maltreatment, are outlined in Table 1. In terms of family context, 76% of the participants had one or more deceased parents, 42% reported taking care of themselves at night, 61% reported hunger (food insufficiency), 63% reported being hit or beaten by their parents, and 21% reported that their parents’ alcohol use had prevented them from providing care. In terms of the participants’ own alcohol and drug use, 34% reported any drunkenness, 9% reported drinking alcohol prior to age 13, and 14% reported any drug use. With regards to their skills, 44% reported that they had no apprenticeship skills. In terms of mental health characteristics, 75% reported sadness and 44% reported that they expect to die before the age of 30.The overall prevalence of reporting violence victimization involving a weapon was 36%, and the prevalence of violence perpetration with a weapon was 19%. In terms of the overlap between victimization and perpetration, 16.6% of youth (11.6% of boys and 24.1% of girls) reported both.
Bivariate associations between demographic and psychosocial correlates and violence experiences are presented in Table 2. Girls were significantly more likely than boys to report victimization only (OR=2.23; 95%CI: 1.33—3.73) and both perpetration and victimization (OR=3.26; 95%CI: 2.12—6.16). Both parental neglect due to alcohol and any self-reported drunkenness were associated with all 3 forms of the outcome variable (perpetration only, victimization only, and both perpetration and victimization). Sadness was also associated with victimization and both perpetration and victimization. Several correlates were specifically associated with both perpetration and victimization including reporting both parents deceased, self-monitoring/care at night, hunger, early alcohol use initiation, any drug use, and sadness.

The multivariate analyses of all correlates are identified in Table 2. Parental neglect due to alcohol use and sadness were significant correlates of victimization only. Reporting hunger, any drunkenness, and any drug use were significantly associated with both perpetration and victimization.
DISCUSSION
In this study of youth living in the slums of Kampala, the findings show that many vulnerable youth, in particularly girls, report both weapon-involved violence perpetration and victimization, which currently is a largely unaddressed issue. While the context for these violent incidences was not assessed, it is clear that the circumstances of these youth living in the slums may present a range of situations involving conflict and altercation with respect to obtaining resources, such as money, food, shelter, and alcohol and drugs. Moreover, these youth reported many adverse childhood experiences and a substantial proportion are orphans with 1 or 2 deceased parents. Thus, the family contexts of these youth are grim and further exacerbated by reports of food insufficiency and limited care, nurturing, or supervision.
In terms of adverse childhood experiences, a substantial proportion of the youth in our study reported having been hit or beaten by their parents and also reported that their parents had been unable to care for them due to their alcohol use, a factor that proved an important correlate of violent victimization in multivariate analyses. Alcohol use is an important concern since estimates indicate that Uganda has one of the highest per capita levels of alcohol consumption in the world.26 Accordingly, parental alcohol abuse appears to be a key concern and perhaps also a contributor to the current living situations for the youth participating in our study.
Among the youth who participated in our study, drunkenness and drug use were significant correlates of reporting both perpetration and victimization involving a weapon. These findings are similar to previous research conducted in the U.S. that underscore the link between a range of alcohol and drug use measures and involvement in violence, as a perpetrator or victim, and also within gang cultures and marginalized youth.27–29 However, as previously mentioned, these youth also experienced a range of adverse experiences and child maltreatment, which may have increased their risk for drinking.30Intriguingly, overall, levels of drinking and early alcohol use initiation prior to age 13 were low among participants when compared to school-attending adolescents in Uganda and Zambia, which may be due to the youth participants in this survey being service-seeking.31,32
In comparing the statistically significant correlates of victimization only, perpetration only and reports of both perpetration and victimization, it is intriguing to note that sadness and parental neglect due to alcohol use were specifically associated only with victimization. In contrast, hunger, drunkenness and drug use were specifically associated with reports of both perpetration and victimization. No correlates were specifically associated with perpetration only, although it should be noted that this category accounted for only 2% of the study sample. Among the study participants, victimization was more frequently reported than perpetration. As such, it may be that the context for either victimization or perpetration of violence involving a weapon may be different and situation-dependent. Because of the scarcity of data on youth who live in the slums and on the streets, it is difficult to make any relevant comparisons of these experiences.
Some limitations restrict the interpretation of the findings of this study. First, the study used a broad definition of street youth, including both homeless youth and youth living in the slums in a variety of living arrangements. Second, because the participants in this study were recruited from UYDEL drop-in centers, the study is based on a convenience sample that may not be generalizable to other populations. Third, the survey instrument used in this study had not been previously piloted among Ugandan youth. However, the majority of the survey items were adopted from previously validated surveys, including the U.S. Youth Risk Behavior Survey24 and the Global School-based Health Survey which has been conducted in Uganda previously.25 Fourth, the low literacy level of many of the study participants required that the survey was read aloud to the participants. The direct face-to-face interaction between the interviewer and the participant may have resulted in underreporting of certain risk behaviors because of social desirability. A fifth limitation is that several study participants provided their responses to survey items in their local language of Luganda, thus requiring the interviewers to translate the answers into English. Sixth, some of the statistical analyses included relatively small sample sizes and yielded relatively wide confidence intervals indicating that findings may be less stable. Lastly, our findings are limited by the cross-sectional nature of this study. A temporal relationship between the psychosocial variables and violence victimization or perpetration cannot be determined, nor can causation be inferred.
Despite these important limitations, the findings from this study describe the prevalence and correlates of relatively severe forms of violence involving a weapon among these vulnerable youth. Hunger, drunkenness, and drug use were the most important factors associated with perpetration and victimization of weapon-involved violence. Because of the scarcity of data related to violence perpetration and victimization among youth in sub-Saharan Africa, additional research is needed to validate these findings. In particular, a longitudinal cohort study would be more suitable to determine the initiation of risk behaviors, as well as contextual factors that may increase risk for involvement in violence. Efforts should also be made to determine modifiable factors that can be incorporated into prevention programs that may reduce, at least partially, the consequences of the adverse childhood experiences experienced by many of these youth.
Footnotes
Supervising Section Editor: Abigail Hankin, MD, MPH
Submission history: Submitted January 17, 2012; Revision received March 13, 2012; Accepted March 14, 2012
Reprints available through open access at http://escholarship.org/uc/uciem_westjem
DOI: 10.5811/westjem.2012.3.11772
Address for Correspondence: Monica H Swahn, PhD, MPH
Georgia State University’s Institute of Public Health, Atlanta, Georgia.
Email: mswahn@gsu.edu.
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Krug EG, Mercy JA, Dahlberg LL, et al. The world report on violence and health. The Lancet.2002;360:1083–8.
2. World Health Organization. World report on violence and health. Geneva: WHO;; 2002.
3. Brown DW, Riley L, Butchart A, et al. Exposure to physical and sexual violence and adverse health behaviors in African children: results from the Global School-based Student Health Survey. Bulletin of the World Health Organization. 2009;87:447–55. [PMC free article] [PubMed]
4. Reza A, Mercy J, Krug E. Epidemiology of violent deaths in the world. Inj Prev. 2001;7:104–11.[PMC free article] [PubMed]
5. Young people and HIV/AIDS: opportunity in crises. New York, NY: UNICEF; 2002. United Nations Children’s Fund.
6. Assistance for Orphans and Other Vulnerable Children in Developing Countries Act. 2005
7. United Nations Children’s Fund. The state of the world’s children: maternal and newborn health.New York, NY; UNICEF: 2009.
8. Whetten K, Ostermann J, Whetten R, et al. More than the loss of a parent: potentially traumatic events among orphaned and abandoned children. Journal of Traumatic Stress. 2011;24:174–82.[PubMed]
9. Mufune P. Street youth in southern Africa. International Social Science Journal. 2000;52:233–43.
10. Swahn MH, Bossarte R, Elimam D, et al. Prevalence and correlates of suicidal ideation and physical fighting: a comparison between students in Botswana, Kenya, Uganda, Zambia and the USA.International Journal of Public Health. 2010;2:195–206.
11. Densley MK, Joss DM. Street children: causes, consequences, and innovative treatment approaches.Work. 2000;15:217–26. [PubMed]
12. Jacob WJ, Smith TD, Hite SJ, et al. Helping Uganda’s street children. Journal of Children and Poverty. 2004;10:3–22.
13. Le Roux J, Smith CS. Causes and characteristics of the street child phenomenon: a global perspective. Adolescence. 1998;33:683–8. [PubMed]
14. Sethi S. European report on preventing violence and knife crime among young people. Geneva: WHO;; 2010.
15. De Benitez S. State of the world’s street children: violence. London: Consortium for Street Children;; 2007.
16. Resnick MD, Ireland M, Borowsky I. Youth violence perpetration: what protects? what predicts? findings from the National Longitudinal Study of Adolescent Health. Journal of Adolescent Health.2004;35 424e1-10.
17. Swahn M, Bossarte R, Gaylor E, et al. Hunger and risk for emotional and behavioral problems: a comparison between students in Botswana, Kenya, Uganda and Zambia. International Public Health Journal. 2010;2:185–94.
18. Olley B. Social and health behaviors in youth of the streets of Ibadan, Nigeria. Child Abuse & Neglect. 2006;30:271–82. [PubMed]
19. Swahn MH. Integrating violence prevention research: examining perpetration and victimization of violence within and across relationship contexts. Archives of Pediatrics and Adolescent Medicine.2010;164:1169–70. [PubMed]
20. Swahn MH, Simon TR, Hertz MF, et al. Linking dating violence, peer violence, and suicidal behaviors among high-risk youth. American Journal of Preventive Medicine. 2008;34:30–8. [PubMed]
21. Worldwatch Institute. Uganda on track to have world’s highest population growth. 20112012Available at: http://www.worldwatch.org/node/4525. Accessed January 15.
22. Munene J, Nambi J. Understanding and helping street children in Uganda. Community Development Journal. 1996;31:343–50.
23. Uganda Youth Development Link (UYDEL) 2012 website. Available at: http://www.uydel.org/. Accessed January 10.
24. Centers for Disease Control and Prevention. Youth risk behavior surveillance–United States, 2005.MMWR. 2006;55:1–108.
25. Centers for Disease Control and Prevention. Global School-based Health Survey online data. 2012Available at: http://www.cdc.gov/GSHS/. Accessed January 15.
26. World Health Organization. Global status report: alcohol policy. Geneva: WHO, Department of Mental Health and Substance Abuse;; 2004.
27. Brewer RD, Swahn MH. Binge drinking and violence. JAMA. 2005;294:616–8. [PubMed]
28. Swahn MH, Bossarte RM, West B, et al. Alcohol and drug use among gang members: experiences of adolescents who attend school. Journal of School Health. 2010;80:353–60. [PubMed]
29. Swahn MH, Bossarte RM, Sullivent EE. Age of alcohol use initiation, suicidal behavior, and peer and dating violence victimization and perpetration among high-risk, seventh-grade adolescents. Pediatrics.2008;121:297–305. [PubMed]
30. Hamburger ME, Leeb RT, Swahn MH. Childhood maltreatment and early alcohol use among high-risk adolescents. Journal of Studies on Alcohol and Drugs. 2008;69:291–5. [PubMed]
31. Swahn MH, Ali B, Palmier J, et al. Alcohol marketing, drunkenness, and problem drinking among Zambian youth: findings from the 2004 Global School-Based Student Health Survey. Journal of Environmental and Public Health. 2011 Article ID 497827.
32. Swahn MH, Ali B, Palmier J, et al. Early alcohol use and problem drinking among students in Zambia and Uganda. Journal of Public Health in Africa. 2011;2:83–86.