
{kind=link}
| Author | Affiliation |
|---|---|
| Jeff Riddell, MD | Department of Emergency Medicine, University of California San Francisco-Fresno, Fresno, California |
| Aaron Case, MD | Department of Emergency Medicine, Oregon Health Sciences University, Portland, Oregon |
| Ross Wopat, MD | Department of Surgery, Oregon Health Sciences University, Portland, Oregon |
| Stephen Beckham, MD | Keck School of Medicine, University of Southern California, Los Angeles, California |
| Mikael Lucas, MD | Keck School of Medicine, University of Southern California, Los Angeles, California |
| Christian D. McClung, MD | Department of Emergency Medicine, Los Angeles County + University of Southern California Medical Center, Los Angeles, California |
| Stuart Swadron, MD | Keck School of Medicine, University of Southern California, Los Angeles, California |
Introduction
Methods
Results
Discussion
Limitations
Conclusion
ABSTRACT
Introduction
Non-contrast computed tomography (CT) is widely regarded as the gold standard for diagnosis of urolithiasis in emergency department (ED) patients. However, it is costly, time-consuming and exposes patients to significant doses of ionizing radiation. Hydronephrosis on bedside ultrasound is a sign of a ureteral stone, and has a reported sensitivity of 72–83% for identification of unilateral hydronephrosis when compared to CT. The purpose of this study was to evaluate trends in sensitivity related to stone size and number.
Methods
This was a structured, explicit, retrospective chart review. Two blinded investigators used reviewed charts of all adult patients over a 6-month period with a final diagnosis of renal colic. Of these charts, those with CT evidence of renal calculus by attending radiologist read were examined for results of bedside ultrasound performed by an emergency physician. We included only those patient encounters with both CT-proven renal calculi and documented bedside ultrasound results.
Results
125 patients met inclusion criteria. The overall sensitivity of ultrasound for detection of hydronephrosis was 78.4% [95% confidence interval (CI)=70.2–85.3%]. The overall sensitivity of a positive ultrasound finding of either hydronephrosis or visualized stones was 82.4% [95%CI: 75.6%, 89.2%]. Based on a prior assumption that ultrasound would detect hydronephrosis more often in patients with larger stones, we found a statistically significant (p=0.016) difference in detecting hydronephrosis in patients with a stone ≥6 mm (sensitivity=90% [95% CI=82–98%]) compared to a stone <6 mm (sensitivity=75% [95% CI=65–86%]). For those with 3 or more stones, sensitivity was 100% [95% CI=63–100%]. There were no patients with stones ≥6 mm that had both a negative ultrasound and lack of hematuria.
Conclusion
In a population with CT-proven urolithiasis, ED bedside ultrasonography had similar overall sensitivity to previous reports but showed better sensitivity with increasing stone size and number. We identified 100% of patients with stones ≥6 mm that would benefit from medical expulsive therapy by either the presence of hematuria or abnormal ultrasound findings.
INTRODUCTION
Computed tomography (CT) is widely accepted as a gold standard imaging modality for the detection of renal calculi and hydronephrosis.1 Unfortunately, CT is costly, adds time to the total emergency department (ED) visit and exposes patients to ionizing radiation. This last factor is of particular concern as renal calculi tend to recur and the mutagenic risks of radiation are cumulative in patients who undergo multiple studies.2,3
In contrast, ultrasound (US) is non-invasive, can be performed quickly at the bedside and emits no ionizing radiation. Focused bedside renal US for the detection of hydronephrosis by emergency physicians (EP) is an established practice and is now integrated within the core emergency medicine curriculum of residency training programs.4 The finding of hydronephrosis on emergency bedside US is an indirect sign of a ureteral stone and has a reported sensitivity of 72–83% when compared to CT.5,6
The presence of hydronephrosis on US in the clinical setting of suspected renal colic can provide sufficient information to guide the treatment and disposition of the patient, obviating the need for further imaging.7,8 Nonetheless, CT imaging, alone or in addition to bedside US, remains near-universal in the evaluation of patients with suspected renal colic in the United States.
Because rates of spontaneous stone passage (e.g., without medical or surgical intervention) are closely correlated to stone diameter, treatment algorithms often hinge upon stone size as a branch point in decision making. The purpose of this study was twofold. First, we aimed to determine the overall sensitivity of bedside US performed by EPs and to compare this to previously reported sensitivities. Second, we sought to determine how sensitivity varied with stone size and number.
METHODS
Study Design and Setting
We performed a structured, explicit, retrospective chart review, closely following previously published criteria for medical record reviews.9,10 The study was based at an urban academic ED with an annual census of approximately 160,000 patient visits and was approved in advance by the local institutional review board committee.
Selection
All adult patients (≥18 years) from July 1, 2009, to January 31, 2010, with an ED diagnosis of renal colic were queried. ICD-9 codes including kidney calculus (592.0), ureter calculus (592.1), urinary calculus unspecified (592.9), bladder calculus (594.1), ureteral calculus (594.2) and renal colic (788.0) were included. Of these charts, those with a CT from the selected visit showing evidence of renal calculus by attending radiologist read were examined for results of bedside US performed by a resident or attending EP during the same visit. All bedside US studies in the ED are performed by EPs who have successfully completed a 2-day course in bedside US. Only those patient encounters with both CT-proven renal calculi and documented bedside US results from the same ED visit were included. Patients were excluded for no other reasons.
Methods of Measurement
We used a set of precise operational definitions of relevant variables. An ultrasound was considered positive if the EP recorded a notation of hydronephrosis [e.g., mild, moderate, severe, small, stage I, stage II, or stage III] or if there was a documented finding of sonographically evident stones. The number of stones was recorded from attending radiologist CT read. When a specific number was not given, we interpreted the words “several,” “few,” and “multiple” as ≥3. In patients with multiple stones, we used the size of the largest stone recorded by attending radiologist read.
Data Collection and Processing
Abstractors were trained during dedicated sessions using mock medical records. Two investigators, each blinded to the study hypothesis, used a standard data abstraction form to independently review charts. The abstractors’ performance was monitored by a third investigator throughout the data abstraction process by reviewing the computerized database for invalid entries. To ensure good inter-rater reliability, we independently screened a random sample of 5% of the study records by both reviewers and compared for all data fields. Inter-rater reliability was 100%. For each patient, an electronic copy of the written ED chart, electronic laboratory results, electronic radiology reports, and electronic clinic follow-up notes were reviewed when available. We resolved coding conflicts by consensus among the authors.
Primary Data Analysis
We compared the final CT report and the results of bedside US demonstrating either hydronephrosis or sonographically visible stones. We used STATA 10 software (College Station, TX) to analyze data. We estimated that a sample size of 100 patients would be necessary to establish a sensitivity of 80.0% and 200 patients for a sensitivity of 90.0%, respectively, assuming 100% prevalence of ureteral stones.11 Sensitivity of ultrasound is reported with 95% confidence intervals. The differences between sensitivity for larger stones versus smaller stones were done using two-sample test of proportions with the a priori condition that the difference would be greater than zero (Ha diff >0). We used a chi-squared test for trend to evaluate the relationship between stone number and sensitivity of ultrasound.
RESULTS
There were 511 subjects during the study period with a diagnosis of renal colic, of which 198 subjects had CT-proven stones. One hundred twenty-five subjects had both CT-proven stones and documentation of a bedside ultrasound performed by the treating physician; this is our study population (Table 1).
Table 1. Characteristics of study subjects.
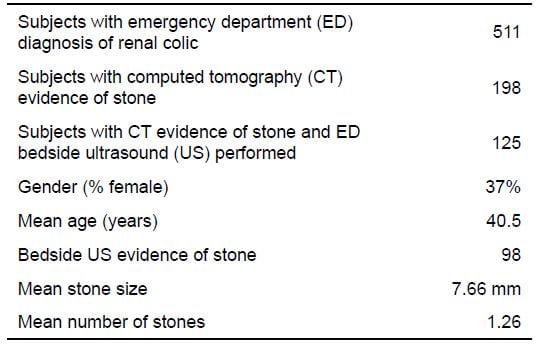
The prevalence of US detection of hydronephrosis was 78.4% (95% CI: 70.2, 85.3%). There were 5 subjects with a stone size greater than 10 mm and absence of hydronephrosis on bedside ultrasound. Stones were visualized on ultrasound among 8.8% (95% CI: 3.8%, 13.8%) of subjects. The overall sensitivity of a positive ultrasound finding of either hydronephrosis or visualized stones was 82.4% (95% CI:75.6%, 89.2%) (Table 2).
Table 2. Sensitivity of ultrasound (US) in all patients.
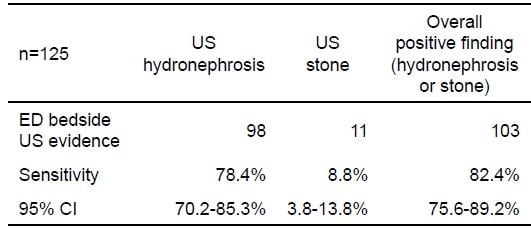
ED, emergency department; CI, confidence interval
Based on a prior assumption that US would detect abnormalities more often in patients with larger stones, we found a statistically significant difference (p=0.016) in patients with a stone ≥6 mm (sensitivity=90% 95% CI=82%–98%]) compared to a stone <6 mm (sensitivity=75% [95% CI=65%, 86%]) (Table 3). For those with 3 or more stones, sensitivity was 100% (95% CI=63–100%). Sensitivity in patients with 2 stones was 94% (95% CI=82%–100%) and 75% (95% CI=65–83%) with a single stone (Table 4). The chi-squared test for trend was statistically significant (p=0.048).
Table 3. Sensitivity of ultrasound (US) by stone size.
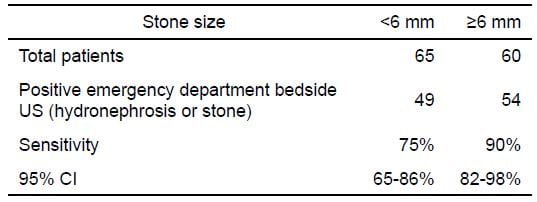
CI, confidence interval
Table 4. Sensitivity of ultrasound (US) by stone number.
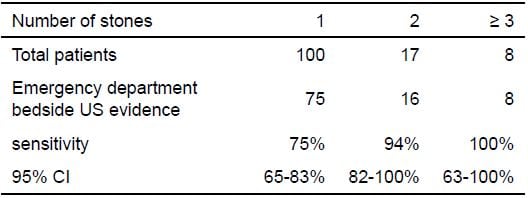
CI, confidence interval
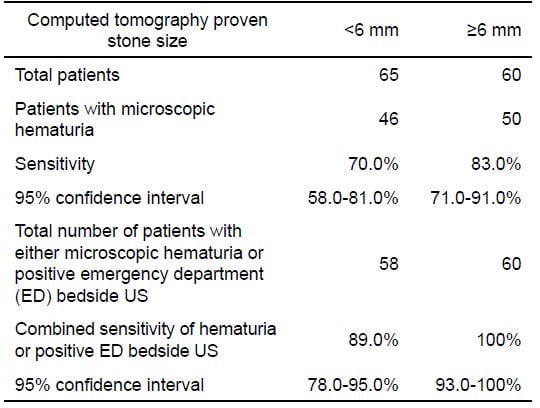
Microscopic hematuria was absent in 23% of cases, including 4 patients with stones greater than 10 mm in diameter. When combining both microscopic hematuria or positive ED bedside ultrasound, sensitivity improved based on stone size from 89% (95% CI=78%–95%) in patients with a stone <6 mm to 100% (95% CI=93%–100%) in patients with a stone ≥6 mm. All patients with a stone size greater than 5 mm had either a positive ultrasound or microscopic hematuria (Table 5).
Table 5. Sensitivity of either hematuria or ultrasound by stone size.
DISCUSSION
Historically, ultrasound has been shown to be effective in guiding the diagnosis and management of suspected renal colic. Kartal et al7 showed that more than 50% of patients with acute flank pain were safely discharged from the ED without further investigations based on urinalysis and hydronephrosis on bedside US. Using a combination of IVP, CT, or passage of stone as the standard, bedside US showed a sensitivity of 81% for the detection of hydronephrosis in the setting of renal colic. Using a similar standard, Rosen et al.5 found a sensitivity of 72%. When using the CT read of the attending radiologist as the gold-standard, Gaspari and Horst6 showed bedside US to be 83% sensitive.
In our study, 100% of patients with stones ≥6 mm were identified by either the presence of hematuria or abnormal bedside US findings. Moreover, we have demonstrated that the sensitivity of bedside US improves with increasing stone size and number. We are unaware of any previous studies looking at statistical trends in sensitivity of EP-performed bedside US based on size or number of stones. Because stones ≥6 mm are less likely to pass, the improving sensitivity of US with larger stones may help EPs select patients that require treatment.12,13 Prospective studies, however, are needed to better define the test characteristics of bedside US in the emergency management of patients with undifferentiated flank pain.
In a recent study that used bedside US as part of an algorithm to evaluate patients with suspected renal colic, Kartal et al7 found that 11 of 27 patients with both negative urine results and the absence of hydronephrosis on ED bedside US had stones demonstrated on subsequent pyelography or CT imaging. However, they did not include stone size in their analysis. In our study, patients without evidence of stones on ED bedside US and without hematuria could be safely assumed to have stones less than 6 mm if detected on CT. Given that these smaller stones typically do not require surgical intervention and do not appear to benefit from medical expulsive therapy, we hypothesize that clinical assessment followed by urinalysis and bedside US could obviate the need for CT in this subset of patients.14
LIMITATIONS
Limitations of our paper include those inherent in any retrospective chart review performed at a single institution. Although we used strict criteria for our chart review, incomplete documentation, missing charts, unrecoverable or unrecorded information, difficulty interpreting acronyms, and variance in the quality of information recorded are all limitations.
Our cohort includes only patients with a final diagnosis of renal colic and not all patients presenting to the ED with flank pain. Inclusion of patients with CT-proven stones only may have introduced bias. Over half of the patients with a diagnosis of renal colic did not receive CT imaging; those who did may have had more severe symptoms and subsequently a higher grade of obstruction. This may have led to an overestimation of the frequency of hydronephrosis. Nonetheless, our reported sensitivities compare favorably to prior published studies.
We based US data only on what was recorded in the chart, so it is possible that some of the 73 patients with no record of US received one that was not documented. Although all EPs performing bedside US met a minimum standard for training, there was significant variation in the US experience among them. Finally, patient characteristics, such as body habitus or body mass index, were not considered and may have limited the both the acquisition and interpretation of CT and bedside US studies.
CONCLUSION
In our population with CT-proven urolithiasis, ED bedside ultrasonography had similar overall sensitivity to previous reports but showed better sensitivity with increasing stone size and number. We identified 100% of patients with stones ≥6 mm that would benefit from medical expulsive therapy by either the presence of hematuria or abnormal ultrasound findings.
Footnotes
Address for Correspondence: Jeff Riddell, MD. University of California San Francisco-Fresno, 155 N Fresno St., Fresno CA, 93701. Email: jriddell@fresno.ucsf.edu. 2 / 2014; 15:96 – 100
Submission history: Revision received January 14, 2013; Submitted June 23, 2013; Accepted September 11, 2013
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Teichman J. Clincal Practice, Acute renal colic from ureteral calculus. New Engl J Med.2004;350:684–693. [PubMed]
2. Broder J, Bowen J, Lohr J, et al. Cumulative CT exposures in emergency department patients evaluated for suspected renal colic. J Emerg Med. 2007;33:161–168. [PubMed]
3. Brenner DJ, Hall EJ. Computed tomography-an increasing source of radiation exposure. N Engl J Med. 2007;357:2277–2284. [PubMed]
4. Perina DG, Brunett PH, Caro DA, et al. EM Model Review Task Force, 2011 Revision. Acad Emerg Med. 2012;19:e19–40. [PubMed]
5. Rosen CL, Brown DF, Sagarin MJ, et al. Ultrasonography by emergency physicians in patients with suspected ureteral colic. J Emerg Med. 1998;16:865–870. [PubMed]
6. Gaspari RJ, Horst K. Emergency ultrasound and urinalysis in the evaluation of flank pain. Acad Emerg Med. 2005;12:1180–1184. [PubMed]
7. Kartal M, Eray O, Culbant A, et al. Prospective validation of a current algorithm including bedside US performed by emergency physicians for patients with acute flank pain suspected renal colic. J Emerg Med. 2006;30:248. [PMC free article] [PubMed]
8. Henderson SO, Hoffner RJ, Aragona JL, et al. Bedside emergency department ultrasonography plus radiography of the kidneys, ureters, and bladder vs intravenous pyelography in the evaluation of suspected ureteral colic. Acad Emerg Med. 1998;5:666–671. [PubMed]
9. Worster A, Bledsoe RD, Cleve P, et al. Reassesing the methods of medical record review studies in emergency medicine research. Ann Emerg Med. 2005;45:448–451. [PubMed]
10. Gilbert EH, Lowenstein SR, Kozoil-McLain J, et al. Chart reviews in emergency medicine research: where are the methods? Ann Emerg Med. 1996;27:305–308. [PubMed]
11. Carly S, Dosman S, Jones SR, et al. Simple nomograms to calculate sample size in diagnostic studies. Emerg Med J. 2005;22:180–181. [PMC free article] [PubMed]
12. Dellabella M, Milanese G, Muzzonigro G. Randomized trial of the efficacy of tamsulosin, nifedipine and phloroglucinol in medical expulsive therapy for distal ureteral calculi. J Urol. 2005;174:167–172.[PubMed]
13. Coll DM, Varanelli MJ, Smith RC. Relationship of spontaneous passage of ureteral calculi to stone size and location as revealed by unenhanced helical CT. Am J Roentgenol. 2002;178:101–103.[PubMed]
14. Ferre RM, Wasielewski JN, Strout TD, et al. Tamsulosin for ureteral stones in the emergency department: a randomized, controlled trial. Ann Emerg Med. 2009;54:432–439. [PubMed]