
{kind=link}
| Author | Affiliation |
|---|---|
| Robert J. Hoffman, MD, MS | Beth Israel Medical Center, Albert Einstein College of Medicine, Department of Emergency Medicine, New York, NY |
| Jefrey R. Dahlen, MD | Beth Israel Medical Center, Albert Einstein College of Medicine, Department of Emergency Medicine, New York, NY |
| Daniela Lipovic, DO | Beth Israel Medical Center, Albert Einstein College of Medicine, Department of Emergency Medicine, New York, NY |
| Kai M. Stürmann, MD | Brookhaven Memorial Hospital Medical Center, East Patchogue, NY |
ABSTRACT
Introduction:
Endotracheal tube cuff (ETTc) inflation by standard methods may result in excessive ETTc pressure. Previous studies have indicated that methods of cuff inflation most frequently used to inflate ETTcs include palpation of the tension in the pilot balloon or injection of a predetermined volume of air to inflate the pilot balloon. If a logarithmic relationship exists between ETTc volume and ETTc pressure, small volumes of additional air will result in dramatic pressure increases after a volume threshold is reached. Our goal was to determine whether the relationship between ETTc volume and ETTc pressure is linear or non-linear.
Methods:
In this Institutional Animal Care and Use Committee-approved study, we recorded ETTc volume and pressure in four anesthetized and mechanically-ventilated canines ranging between 30–40 pounds (mean 34.7lb, SD 3.8lb) that were endotracheally intubated with a 7.0 mm ETT. The varying cuff pressures associated with a distribution of 28 progressively increasing volumes of air in the ETTc were recorded. Spearman correlation was performed to determine if a linear or non-linear relationship existed between these variables.
Results:
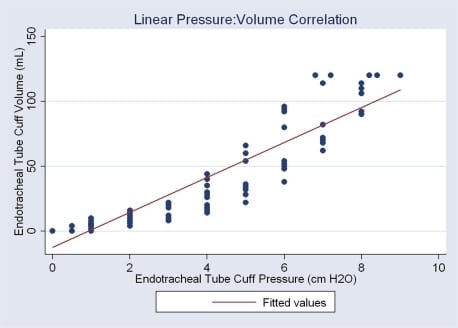
The Spearman rho coefficient of correlation between ETTc volume and ETTc pressure was 0.969, or approximately 97%, suggesting near-perfect linear relationship between ETTc volume and ETTc pressure over the range of volumes and pressures tested.
Conclusion:
Over the range of volumes and pressures tested a linear relationship between volume and pressure results in no precipitous increase in slope of the pressure:volume curve as volume increases.
INTRODUCTION
Endotracheal intubation can be a lifesaving procedure. Endotracheal tube cuffs help prevent air leak around the tube and aspiration of upper airway secretions.1 Risks associated with placement of an endotracheal tube (ETT) include esophageal intubation, aspiration, and cardiac dysrhythmias.2 Excessive or prolonged pressure of the ETTc may cause acute catastrophic airway injury, such as tracheal rupture, or may cause subacute or chronic injury, such as tracheal necrosis, tracheal stenosis, tracheoesophageal fistula, or laryrngeal nerve palsy.
Endotracheal cuffs in the 1960s were made of rubber and classified as high pressure-low volume systems. They commonly required pressures of greater than 100 cm H2O to be inflated. Since these tubes would inflate in a non-circular fashion, they would present with additional complications associated with higher pressures. The most problematic issue was the tip of the ETT directly contacting the trachea, leading to tracheal injury. In the late 1960s the transition to high volume-low pressure cuffs significantly reduced the incidence of tracheal complications. Although high volume-low pressure cuffs have limitations, their safety features surpass the risks involved with low volume-high pressure ETT.3
Various models have been compared to evaluate ETTc pressure thresholds that have an adverse effect on tracheal circulation. A horse model using cuff pressures of 80–100 cm H2O and 120 cm H2O revealed signs of mucosal damage after 175 minutes of intubation. These lesions were less severe in the lower ETTc pressures.4 In a dog model, pressure exceeding 30 cm of H2O for 15 minutes resulted in mucosal injury.5 However, time in excess of 15 minutes did not increase tissue damage with additional exposure. In humans, endotracheal cuff pressures at approximately 30 cm H2O can impair tracheal mucosa perfusion, and a critical perfusion pressure is reached at 50 cm H2O.6 In the 1980s endoscopic studies demonstrated impaired blood flow in the tracheal mucosa at cuff-to-wall pressures of 28–34 cm H2O and complete stoppage of blood flow at pressures greater than 50 cm H2O.7
Studies assessing clinician ability to appropriately inflate an ETTc and assess ETTc pressure in endotracheally intubated patients have been published in recent years.8,9These are congruent in suggesting that clinicians have poor ability to properly inflate ETTc to safe pressures using standard techniques and that ETTc pressures in these patients frequently exceed safe maximum pressures.
METHODS
In this Institutional Animal Care and Use Committee-approved study, we recorded ETTc volumes and pressures in four anesthetized and mechanically-ventilated canines weighing between 30–40 pounds (mean 34.7lb, SD 3.8lb) that were endotracheally intubated with a 7.0 mm ETT (Mallinckrodt, Hazelwood, MO). The varying cuff pressures associated with a distribution of 28 progressively increasing volumes of air in the ETTc were recorded. Endotracheal tube cuff pressure was measured using an analog manometer (Cufflator®, Posey Corporation, Pasadena, CA). This manometer measures pressures in the range of 0 cm H2O to 120 cm H2O in 2 cm increments. Data analysis was performed using Intercooled Stata 8.2 statistical software (Stata Corporation, College Station, TX).
The volumes of air injected were selected on the basis of 1) the minimum volume required to generate any measurable pressure in the ETTc, and 2) the volume associated with approximation of a cuff pressure of 120 cm H2O, above which this manometer is unable to accurately measure pressure. The actual volumes of air injected into the ETTc ranged from 0.5 mL to 9.0 mL of air, and the actual pressures measured ranged from 2 cm H2O to 120 cm H2O.
RESULTS
Spearman rho correlation of the variables of volume and pressure was 0.969, or approximately 97% correlation between volume and pressure. These results suggest a near-perfect linear relationship between ETTc volume and ETTc pressure (Figure).
DISCUSSION
The primary findings of the present study consist of a 97 % correlation between ETTc volume and ETTc pressure in a strongly linear relationship.
Dangers associated with exponential increase of cuff pressure for a given volume of air could include severe tracheal injury. In a study by Svenson et al.1 it was discovered that most ETTc pressures exceeded the recommended limits, and that the time spent in the ED or prehospital setting may be long enough for tracheal damage to occur. Curiel et al.10found that high ETTc pressure is related to post-intubation tracheal pain in patients that underwent elective surgery. However, only duration of intubation, ETTc pressure and tracheal pain were compared.
Results from our study, using four anesthetized and mechanically ventilated canines, demonstrated a near-perfect linear relationship between cuff volume and pressure. Therefore, clinicians and EMS personnel can feel assured that when inflating an ETTc at or even somewhat above appropriate cuff pressure, addition of air to the ETTc should not result in large or precipitous exponential increases in ETTc pressure. It should be noted, however, that the volume of air required to reach 50 cm H2O is only 150% of that required for safe ETTc pressure, suggesting that the margin for error in over inflation is not large.
LIMITATIONS
Potential limitations to our study may include variability in an animal model versus human in vivo conditions, the effect of different size ETTs on the study results, as well as many less concerning variables, such as brand of ETT used, atmospheric conditions, etc. Studies using canine tracheal and upper airways as models are published,11 but most use the tracheal tissue rather than tracheal anatomy as the basis for the model.12,13 Thus, the canine upper airway is not a well-established airway model. Additionally, it is possible that at higher volumes, beyond those tested here, a different relationship might exist.
CONCLUSION
At the volumes and pressures tested, an extraordinarily strong linear correlation was demonstrated in these canines when ETTc volume and pressure were measured. A particularly relevant point is that the correlation between volume and pressure holds at the upper limits of both volume and pressure tested. The significance of these findings is that, due to the strong linear relationship, there is not a precipitous increase in slope of the pressure:volume curve at greater volumes. Injection of additional air while at the upper end of the pressure:volume curve tested does not cause a precipitous rise in ETTc pressure. However, the volume of air required to reach 50 cm H2O is only 150% of that required for safe ETTc pressure, suggesting that the margin for error in overinflation is not large.
Footnotes
Supervising Section Editor: Brandon K. Wills DO, MS
Submission history: Submitted September 11, 2008; Revision Received December 25, 2009; Accepted January 02, 2009
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Robert J. Hoffman, MD, MS, Department of Emergency Medicine, Beth Israel Medical Center, Albert Einstein College of Medicine, 330 East 17th Street, New York, NY 10003
Email: rjhoffman@pol.net
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Svenson JE, Lindsay MB, O’Connor JE. Endotracheal Intracuff Pressures in the ED and Prehospital Setting: Is There a Problem? Am J Emerg Med. 2007;25:53–6. [PubMed]
2. Jaber S, Amraoui J, Lefrant JY, Arich C, Cohendy R, Landreau L, Calvet Y, Capdevila X, Mahamat A, Eledjam JJ. Clinical Practice and Risk Factors for Immediate Complications of Endotracheal Intubation in the Intensive Care Unit: A Prospective, Multiple-Center Study. Crit Care Med. 2006;34:2355–61. [PubMed]
3. Parwani V, Hoffman RJ, Russell A, Bharel C, Hahn IH. Practicing Paramedics Cannot Generate or Estimate Safe Endotracheal Tube Cuff Pressure Using Standard Techniques.Prehosp Emerg Care. 2007;11:307–11. [PubMed]
4. Touzot-Jourde G, Stedman NL, Trim CM. The Effects of Two Endotracheal Tube Cuff Inflation Pressures on Liquid Aspiration and Tracheal Wall Damage in Horses. Vet Anaesth Analg. 2005;32:23–9. [PubMed]
5. Nordin U. Examination of cuff-induced tracheal injuries in experimental animals.Lakartidningen. 1978;75:3554–7. [PubMed]
6. Mann C, Parkinson N, Bleetman A. Endotracheal Tube and Laryngeal Mask Airway Cuff Volume Changes with Altitude: A Rule of Thumb for Aeromedical Transport. Emerg Med J. 2007;24:165–7. [PMC free article] [PubMed]
7. Blanch PD. Laboratory Evaluation of 4 Brands of Endotracheal Tube Cuff Inflator. Resp Care. 2004;49:166–173.
8. Hoffman RJ, Parwani V, Hahn IH. Experienced Emergency Medicine Physicians Cannot Safely Inflate Or Estimate Endotracheal Tube Cuff Pressure Using Standard Techniques.Am J Emerg Med. 2006;24:139–43. [PubMed]
9. Galinski M, Tréoux V, Garrigue B, Lapostolle F, Borron SW, Adnet F. Intracuff Pressures of Endotracheal Tubes in the Management of Airway Emergencies: The Need for Pressure Monitoring. Ann Emerg Med. 2006;47:545–47. [PubMed]
10. Curiel G, Guerrero-Romero F, Rodriguez-Moran M. Cuff Pressure in Endotracheal Intubation: Should it be Routinely Measured? Gac Med Mex. 2001;137:179–82. [PubMed]
11. Martins RH, Braz JR, Defaveri J, Gregorio EA, Abud TM. Effect of high laryngeal mask airway intracuff pressure on the laryngopharyngeal mucosa of dogs. Laryngoscope.2000;110:645–50. [PubMed]
12. Genden EM, Gannon PJ, Smith S, Keck N, Deftereos M, Urken ML. Microvascular transfer of long tracheal autograft segments in the canine model. Laryngoscope.2002;112:439–44. [PubMed]
13. Long CM, Conley SF, Kajdacsy-Balla A, Kerschner JE. Laryngotracheal reconstruction in canines: fixation of autologous costochondral grafts using polylactic and polyglycolic acid miniplates. Otolaryngology — Head & Neck Surgery. 2001;127:570–5.