
{kind=link}
| Author | Affiliation |
|---|---|
| Kaitlyn Schmutz, PA-C | Duke University Hospital, Department of Emergency Medicine, Durham, North Carolina |
| Gaea McGaig, PA-C | Rex Hospital, Department of Emergency Medicine, Raleigh, North Carolina |
| B. Jason Theiling, MD | Duke University School of Medicine, Department of Surgery, Division of Emergency Medicine, Durham, North Carolina |
ABSTRACT
Case Presentation
Approximately 94% of patients with Hirschsprung’s disease (HD) are diagnosed before the age of five. In our case, a young adult with years of constipation presented to the emergency department with significant abdominal distention. He was ultimately diagnosed with HD, which was identified using computed tomography (CT).
Discussion
In HD, we find defects in gastric motility due to improper gut colonization. Without childhood recognition, HD often leads to chronic constipation and failure to thrive in adulthood. CT is a key step in identifying this rare adult diagnosis that should be considered in all patients with a history of chronic constipation.
CASE PRESENTATION
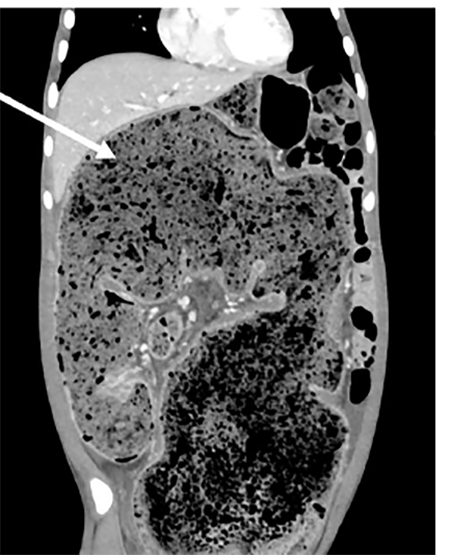
An 18-year-old male with history of chronic constipation (CC) presented to the emergency department complaining of left lower extremity (LLE) swelling and abdominal distention. Despite a daily polyethylene glycol regimen, he had previously required both manual and procedural disimpactions. He was tolerating both solids and liquids without vomiting. He denied infectious symptoms and was afebrile. On examination, his abdomen was distended without tenderness. The LLE had circumferential pitting edema without erythema or tenderness. He underwent computed tomography (CT) of the abdomen and pelvis with intravenous contrast that demonstrated a high degree of colonic distention (Image 1) with mass effect causing hydronephrosis, intrahepatic biliary ductal dilatation, and mesenteric venous engorgement (Image 2).
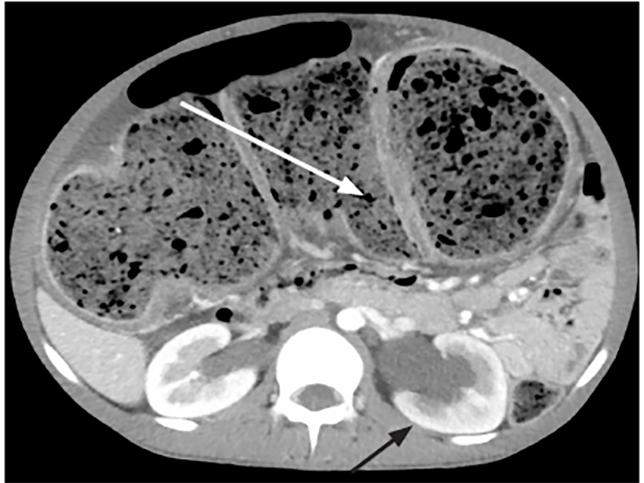
There was also CT evidence of iliac vein compression (left greater than right) that caused his LLE edema. He ultimately underwent colonic decompression followed by colonoscopy and rectal biopsy, which confirmed his diagnosis of Hirschsprung‘s disease (HD).
DISCUSSION
HD occurs in 1:5000 births, but in adults it is rarely considered and often undiagnosed. The pathophysiology of HD is an absence of intramural ganglion cells of the submucosal (Meissner’s) and myenteric (Auerbach’s) neural plexuses, which are situated between smooth muscle layers in the affected bowel segment.1,2 While it is likely that the colonic region proximal to the distal obstructed segment assumes a compensatory role in function for undiagnosed adults, these patients will often still suffer from CC.3 CC has prevalence estimates from 1%–8% in North America with significant impact on quality of life.4 A CT suggestive of HD could lead to complete eradication or significant improvement in CC by confirmational biopsy and definitive surgical management.5 For these reasons, Hirschsprung’s disease should be considered in all adults with refractory constipation.
CPC-EM Capsule
What do we already know about this clinical entity?
Hirschsprung’s disease (HD) is characterized by gastric dysmotility and is associated with neonates.
What is the major impact of the image(s)?
This computed tomography of a young adult patient demonstrates colonic distention with significant mass effect, which was highly suspicious for undiagnosed HD.
How might this improve emergency medicine practice?
While it is a congenital condition, HD can present later in life as chronic constipation and should prompt an expansion of the differential diagnosis.
Footnotes
Section Editor: Manish Amin, DO
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
The authors attest that their institution requires neither Institutional Review Board approval, nor patient consent for publication of this image in emergency medicine. Documentation on file.
Address for Correspondence: B. Jason Theiling, MD, Duke University, Department of Surgery, Division of Emergency Medicine, Box 3096 DUMC, Durham, NC 27710. Email: Jason.theiling@duke.edu. 4:480 – 481
Submission history: Revision received January 10, 2020; Submitted May 28, 2020; Accepted June 1, 2020
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Qiu JF, Shi YJ, Hu L, et al. Adult Hirschsprung’s disease: report of four cases. Int J Clin Exp Pathol. 2013;6(8):1624-30.
2. Heanue TA, Pachnis V. Prospective identification and isolation of enteric nervous system progenitors using Sox2. Stem Cells. 2011;29(1):128-40.
3. Hye JK, Ah YK, Choong WL, et al. Hirschsprung disease and hypoganglionosis in adults: radiologic findings and differentiation. Radiology. 2008;247(2):428-34.
4. Sanchez MI, Bercik P. Epidemiology and burden of chronic constipation. Can J Gastroenterol. 2011;25(Suppl B):11B-5.
5. Chen F, Winston JH, Jain SK, et al. Hirschsprung’s disease in a young adult: report of a case and review of the literature. Ann Diagn Pathol. 2006;10(6):347-51.