
{kind=link}
| Author | Affiliation |
|---|---|
| Jodi Spangler, BA | University of Washington, School of Medicine, Department of Emergency Medicine, Seattle, Washington |
| Jonathan Ilgen, MD | University of Washington, School of Medicine, Department of Emergency Medicine, Seattle, Washington |
ABSTRACT
Case Presentation
A 55-year-old woman with a history of end-stage renal disease, peripheral vascular disease, and multiple prior abdominal surgeries presented to the emergency department with three days of diffuse, severe, abdominal pain with accompanying nausea, emesis, and food intolerance. A computed tomography (CT) of her abdomen demonstrated a “whirl” of small bowel and mesenteric vessels, raising suspicion for mesenteric volvulus and resultant small bowel obstruction.
Discussion
Mesenteric volvulus is a low incidence, high mortality condition; therefore, early recognition and operative intervention are critical. Patients with a “whirl sign” on CT are more likely to require surgical intervention for their small bowel obstruction.
CASE PRESENTATION
A 55-year-old woman with a history of end-stage renal disease, peripheral vascular disease, and multiple prior abdominal surgeries presented to the emergency department with three days of diffuse, severe, abdominal pain with accompanying nausea, emesis, and food intolerance. Her physical examination was remarkable for a soft, slightly distended abdomen with diffuse tenderness to palpation. She had no guarding or rebound. A computed tomography (CT) of her abdomen demonstrated a “whirl” of small bowel and mesenteric vessels (Video), raising suspicion for mesenteric volvulus and resultant small bowel obstruction.1,2
In this patient, an exploratory laparotomy was performed amid concern for small bowel ischemia, and a mesenteric volvulus was confirmed intraoperatively. A small bowel resection with extensive adhesiolysis was performed, and multiple mesenteric lymph nodes were excised. The patient had an unremarkable postoperative course and was discharged home.
DISCUSSION
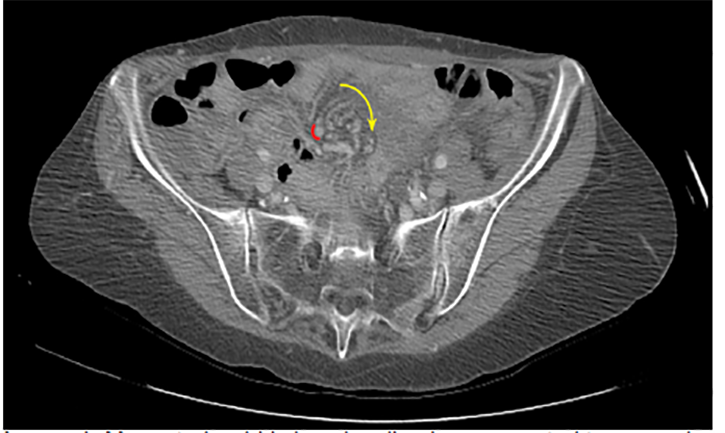
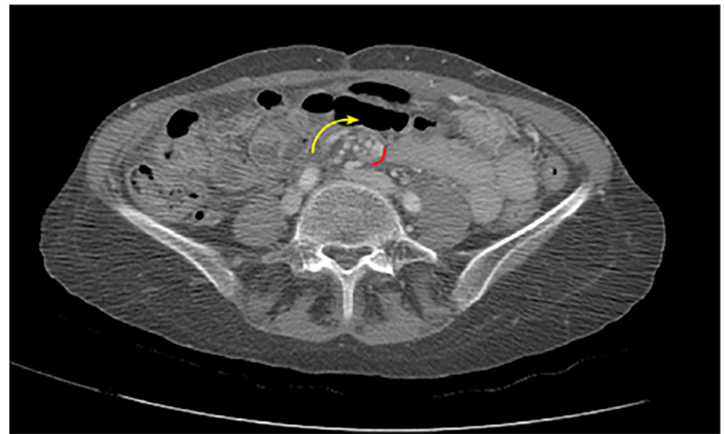
Mesenteric volvuli occur when bowel twists around its mesenteric root.1 This results in bowel wall and vascular compression, with subsequent intestinal obstruction and ischemia. Mesenteric volvuli are classified as “primary” when occurring in the setting of an otherwise normal abdominal cavity, and “secondary” when occurring in the setting of pre-existing lesions such as adhesions or malrotation.3 Abdominal pain is the typical presenting symptom, and despite its low incidence, mortality rates from mesenteric volvuli are high; thus, early recognition and operative intervention are critical.3 The “whirl sign” on CT imaging (Images 1 and 2) is a highly specific finding for intestinal volvulus (albeit poorly sensitive), and should raise suspicion for a closed loop obstruction.4 Presence of the whirl sign is helpful for guiding management of patients with clinical and radiologic signs of small bowel obstruction, as patients with this finding are 25 times more likely to require surgery than those without this finding on imaging.4
CPC-EM Capsule
What do we already know about this clinical entity?
Mesenteric volvulus occurs when bowels twists around its mesenteric root and can result in bowel wall and vascular compression, intestinal obstruction and ischemia.
What is the major impact of the image(s)?
Mesenteric volvulus is a low incidence, high mortality condition. Therefore, early recognition and operative intervention are critical.
How might this improve emergency medicine practice?
Whirl sign is helpful for guiding management of patients with signs of small bowel obstruction, as patients with this finding are more likely to require surgery.
Footnotes
Section Editor: Scott Goldstein, MD
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
Patient consent has been obtained and filed for the publication of this image in emergency medicine.
Address for Correspondence: Jodi Spangler, BA, University of Washington School of Medicine, Department of Emergency Medicine, Harborview Medical Center, 325 9th Ave., Box 359702, Seattle, WA 98104. Email: jspang@uw.edu. 4:470 – 471
Submission history: Revision received January 23, 2020; Accepted March 7, 2020
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Fisher JK. Computed tomographic diagnosis of volvulus in intestinal malrotation. Radiology. 1981;140(1):145-6.
2. Khurana B. The whirl sign. Radiology. 2003;226(1):69-70.
3. Anton R, Leslie WO. Acute small bowel volvulus in adults: sporadic form of strangulating intestinal obstruction. Ann Surg. 1992;216(2):135-41.
4. Duda JB, Bhatt S, Dogra VS. Utility of CT whirl sign in guiding management of small-bowel obstruction. AJR Am J Roentgenol. 2008;191(3):743-7.
SUPPLEMENTARY MATERIAL
Mesenteric whirl sign. Computed tomography of the abdomen demonstrates a swirling mass (see arrow) of soft-tissue and fat attenuation indicative of twisted loops of small bowel and mesenteric vessels.