
{kind=link}
| Author | Affiliation |
|---|---|
| William Weber, MD, MPH | The University of Chicago, Department of Medicine, Section of Emergency Medicine, Chicago, Illinois |
| Jacob Moore, MD | The University of Chicago, Department of Medicine, Section of Emergency Medicine, Chicago, Illinois |
| Navneet Cheema, MD | The University of Chicago, Department of Medicine, Section of Emergency Medicine, Chicago, Illinois |
CASE PRESENTATION
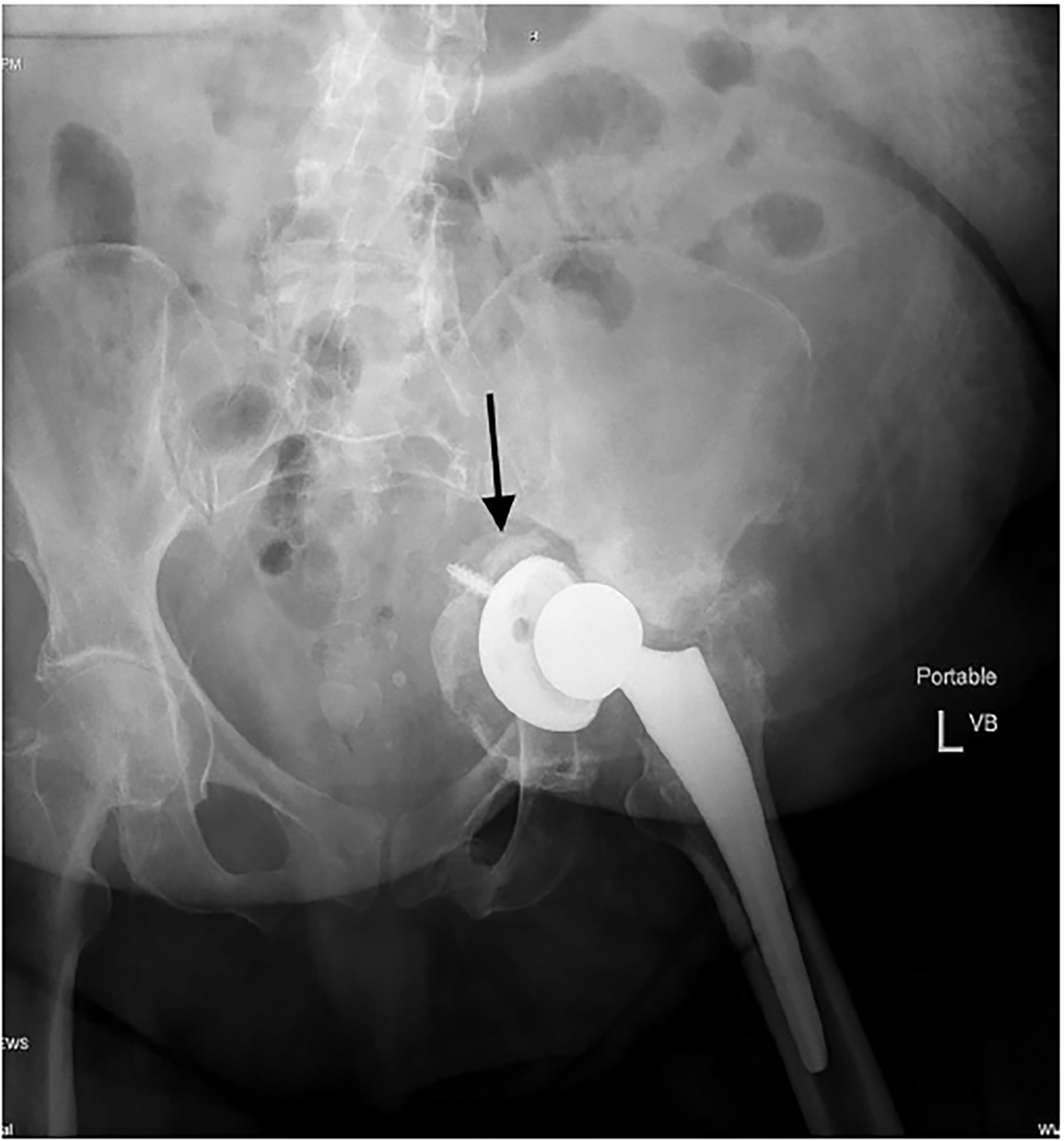
A 69-year-old woman with a history of osteopenia and left total hip arthroplasty three months prior presented from home to the emergency department with leg pain and inability to ambulate. She had fallen from standing onto a tile floor, making contact with her left hip. She was mildly hypertensive, with a blood pressure of 137/92 mmHg and tachycardic, with a heart rate of 105 beats per minute, but had otherwise unremarkable vitals. On examination, she had tenderness and developing ecchymosis over the greater trochanter of the left femur. Her left leg was slightly shortened and externally rotated but neurovascularly intact. A pelvic radiograph (Image) showed medial displacement of the acetabulum and femoral head into the lesser pelvis. Angiography failed to reveal any vascular disruption. She remained hemodynamically stable and was taken to surgery for an urgent but successful internal pelvic fixation.
DIAGNOSIS
Acetabular protrusion most commonly occurs as a chronic erosion of the acetabulum in patients with osteoporosis or other disease of the bone (e.g., osteomalacia, ankylosing spondylitis). Also, as in the case of acute trauma, force transmitted through joint can cause failure of acetabular integrity. This acetabular protrusion brings the femoral head in close proximity to pelvic contents, risking further injury. Providers should assess for sciatic nerve damage, which occurs in up to 30% of acute acetabular fractures, as well as injury to the iliac artery, which is at risk of shearing injury as it courses along the internal pelvic cavity.2 Unlike with other pelvic fractures, there is no role for pelvic binding in acetabular protrusion, as it can potentially worsen neurovascular damage.3 For the hemodynamically unstable patient, interventional radiology should be consulted for embolization of the internal iliac.4 Stable patients may be placed in traction to minimize medial force on the acetabulum.
Documented patient informed consent and/or Institutional Review Board approval has been obtained and filed for publication of this case report.
CPC-EM Capsule
What do we already know about this clinical entity?
Acetabular protrusion is a medial displacement of the acetabulum into the true pelvis. It usually occurs chronically, as natural forces cause the femoral head to erode through weakened bone.
What is the major impact of the image(s)?
Acute traumatic protrusion jeopardizes nearby structures, including iliac vessels. Traditional pelvic binding increases risk of neurovascular injury, acute hemorrhage, and limb ischemia.
How might this improve emergency medicine practice?
Physicians encountering traumatic acetabular protrusion should avoid pelvic binding, and have low threshold to consult interventional radiology for angiography and possible embolization.
Footnotes
Section Editor: Manish Amin, DO
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
Address for Correspondence: William Weber, MD, MPH, The University of Chicago, Department of Medicine, Section of Emergency Medicine, 5841 S. Maryland Avenue, MC5068, Room L539 Chicago, IL 60637. Email: williamdanielweber@gmail.com. 2:260 – 261
Submission history: Revision received January 29, 2018; Submitted March 23, 2018; Accepted March 28, 2018
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. McBride MT, Muldoon MP, Santore RF, et al. Protrusio acetabuli: diagnosis and treatment. J Am Acad Ortho Surg. 2001;9(2):79-88.
2. Issack PS, Helfet DL. Sciatic nerve injury associated with acetabular fractures. HHS J. 2009;5(1):12-8.
3. Auston DA, Simpson RB. Initial treatment of “pelvic injuries” with commercially available pelvic binders results in displacement of acetabular fractures. JBJS Case Connect. 2015;5(1):e:20-e4.
4. Lopera JE. Embolization in trauma: principles and techniques. Semin Intervent Radiol. 2010;27(1):14-28.