
{kind=link}
| Author | Affiliation |
|---|---|
| Shawn Catmull, DO | Kingman Regional Medical Center, Department of Emergency Medicine, Kingman, Arizona |
| John Ashurst, DO, MSc | Kingman Regional Medical Center, Department of Emergency Medicine, Kingman, Arizona |
ABSTRACT
Tethered spinal cord syndrome refers to signs and symptoms of motor and sensory dysfunction related to increased tension on the spinal cord due to its abnormal attachment; it has classically been associated with a low-lying conus medullaris. Treatment is primarily surgical and has varying degrees of results. Although rarely diagnosed in the emergency department, the emergency physician must be aware of the disease in patients presenting with signs and symptoms concerning for cauda equina syndrome.
CASE PRESENTATION
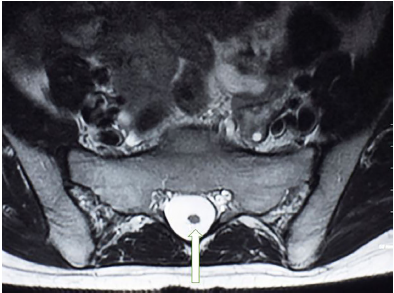
A 30-year-old male presented to the emergency department with a three-day history of low back pain associated with urinary incontinence. His past medical history was significant for numerous urinary tract infections and bilateral hydronephrosis with associated mega-ureters status post ureteral stenting. Physical examination revealed tenderness to palpation along the paravertebral musculature of the lower back, normal muscle strength and tone, normal sphincter tone and no paresthesia along any dermatome. Magnetic resonance imaging (MRI) of the lumbar spine was obtained and depicted a dorsally positioned spinal cord segment within the spinal canal that continued to the position of the fifth lumbar and first sacral vertebrae (Images 1 and 2). The patient’s case was discussed with the neurosurgical services and he underwent surgical decompression as an outpatient. The patient had complete resolution of his urinary symptoms following the procedure.

DIAGNOSIS
Tethered spinal cord syndrome (TCS), first described in 1857, is a neurological disorder caused by an abnormal attachment of the spinal cord to surrounding tissues.1,2 TCS can be caused by congenital (primary) or acquired (secondary) disorders.1,2 Congenital disorders can occur anytime during embryologic development.1,2 Acquired TCS can occur from lipomas, abnormal dural tracts, infections, or trauma.1,2 The most common physical exam finding in adult patients with TCS is low back pain with flexion, but other neurologic findings including weakness, paresthesia, gait abnormalities, and incontinence may occur.1-3 In those suspected of TCS, the spine should be examined for any signs of spina bifida and scoliotic deformities and the feet should be examined for any signs of clubbing.1,2 MRI is currently the gold standard for diagnosis, and neurosurgical intervention is the treatment of choice.1,2
CPC-EM Capsule
What do we already know about this clinical entity?
Tethered cord syndrome is a rare cause of back pain that is caused by an abnormal attachment of the spinal cord to surrounding tissues.
What is the major impact of the image(s)?
The image depicts the conus medullaris below the typical anatomical location that is expected by the emergency physician (EP). The EP should be aware of anatomical variants for the future treatment of patients.
How might this improve emergency medicine practice?
The EP should keep a broad differential when faced with a patient with back pain and frequent urinary tract infections.
Footnotes
Section Editor: Shadi Lahham, MD
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
Documented patient informed consent and/or Institutional Review Board approval has been obtained and filed for publication of this case report.
Address for Correspondence: John Ashurst, DO, MSc, Kingman Regional Medical Center, Department of Emergency Medicine, 3269 Stockton Hill Road, Kingman, AZ 86409. Email: ashurst.john.32.research@gmail.com. 3:297 – 298
Submission history: Revision received January 27, 2019; Submitted April 10, 2019; Accepted April 22, 2019
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. Dr. Ashurst serves as a Section Editor for CPC-EM.
REFERENCES
1. Agarwalla PK, Dunn IF, Scott RM, et al. Tethered cord syndrome. Neurosurg Clin N Am. 2007;18(3):531-47.
2. Hertzler DA, DePowell JJ, Stevenson CB, et al. Tethered cord syndrome: a review of the literature from embryology to adult presentation. Neurosurg Focus. 2010;29(1):E1.
3. Akay KM, Ersahin Y, Cakir Y. Tethered cord syndrome in adults. Acta Neurochir (Wien). 2000;142(10):1111-5.