
{kind=link}
| Author | Affiliation |
|---|---|
| Jamie Adamski, DO | Jefferson Northeast, Department of Emergency Medicine, Philadelphia, Pennsylvania |
| Divya Mohan, DO | Jefferson Northeast, Department of Emergency Medicine, Philadelphia, Pennsylvania; Jefferson Northeast, Department of Family Medicine, Philadelphia, Pennsylvania |
| Christopher Waasdorp, DO | Jefferson Northeast, Department of Emergency Medicine, Philadelphia, Pennsylvania; Jefferson Northeast, Department of Family Medicine, Philadelphia, Pennsylvania |
ABSTRACT
Phrygian cap and its rare relative, pseudo-duplication of the gallbladder, are two radiologic findings that may be revealed on ultrasound evaluation. Correct identification of Phrygian cap and pseudo-duplication should trigger a careful survey of the gallbladder in its entirety to rule out pathology. These anatomic variants may lead to partial under-distension of the gallbladder and can cause the gallbladder wall to appear falsely thickened. Asymptomatic patients with this finding may be safely discharged while symptomatic patients may require further surgical consultation.
CASE PRESENTATION
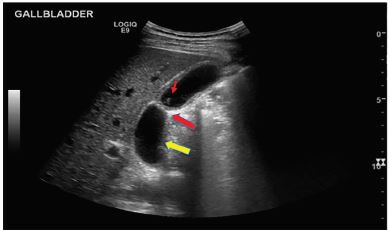
A 30-year-old male with history of cholelithiasis presented with right upper and lower quadrant abdominal pain, nausea, vomiting, and subjective fevers. He denied diarrhea, hematochezia, melena, dysuria, hematuria, urinary frequency, chest pain, or shortness of breath. History raised suspicion for cholecystitis versus appendicitis. Labs revealed a mild leukocytosis. Computed tomography showed gallbladder wall thickening (Image 1), and point-of-care ultrasound (Image 2) demonstrated a Phrygian cap with pseudo-duplication of the gallbladder. After surgical consultation, cholescintigraphy was negative for cholecystitis. With successful pain control and oral fluid challenge, the patient was discharged with outpatient surgical follow-up.

DISCUSSION
Correct identification of Phrygian cap and its rare relative, pseudo-duplication of the gallbladder, warrants careful survey of the gallbladder to rule out underlying pathology.2 The term Phrygian cap refers to a portion of the gallbladder that contains an outpouching or folded-over portion. Pseudo-duplication of the gallbladder, a congenital abnormality with an incidence of 1:4000, refers to a duplicate appearance of the gallbladder in the presence of a Phrygian cap. Pseudo-duplication of the gallbladder is associated with congenital biliary obstruction and is important to identify, as the distal segment past the “fold” of the Phrygian cap may be relatively under-distended. This under-distension may allow the gallbladder wall to appear falsely thickened. In an asymptomatic patient, Phrygian cap has no pathological significance and prophylactic cholecystectomy is not necessary. However, in symptomatic patients, further evaluation and surgical consultation may be indicated.4 Correct identification of these anatomic variants is important to avoid misidentifying a thickened wall as pathologic in an otherwise normal gallbladder.3,4
CPC-EM Capsule
What do we already know about this clinical entity?
In a patient with right upper quadrant pain, it is important to distinguish a diseased gallbladder from a healthy one.
What is the major impact of the image(s)?
Correct identification of two anatomic variants in the gallbladder, Phyrgian cap and pseudo-duplication, will help determine whether or not a gallbladder is diseased.
How might this improve emergency medicine practice?
Using ultrasound to identify normal anatomy and anatomic variants aids in distinguishing a diseased versus a healthy gallbladder and determining appropriate treatment.
Footnotes
Section Editor: John Ashurst, DO
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
Documented patient informed consent and/or Institutional Review Board approval has been obtained and filed for publication of this case report.
Address for Correspondence: Divya Mohan, DO, Jefferson Northeast, Department of Emergency Medicine, 108000 Knights Rd, Philadelphia, PA 19114. Email: dxm289@jefferson.edu. 4:103 – 104
Submission history: Revision received April 5, 2019; Submitted September 3, 2019; Accepted September 6, 2019
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Kannan N, Kannan U, Ganesh Babu C. Congenital bilobed gallbladder with Phrygian cap presenting as calculus cholecystitis. J Clin and Diagn Research. 2014;8(8):ND05-6.
2. Dalal S, Chauhan T, Kumar R, et al. Pseudo-duplication of the gall bladder due to Phrygian cap: a case report. Internet J Surg. 2013;29(1):1-3.
3. Meilstrup JW, Hopper KD, Thieme GA. Imaging of gallbladder variants. AJR Am J Roentgenol. 1991;157(6):1205-8.
4. Van Kamp MJSV, Bouman DE, Steenvoorde P, et al. A Phrygian cap. Case Rep in Gastro. 2013;7(2):347-51.