
{kind=link}
| Author | Affiliation |
|---|---|
| Fadwa Al Hammadi, MBBS | Sheikh Khalifa Medical City, Department of Emergency Medicine, Abu Dhabi, United Arab Emirates |
| Rasha Buhumaid, MBBS | Mohammed Bin Rashid University of Medicine and Health Sciences, Department of Emergency Medicine, Dubai, United Arab Emirates |
ABSTRACT
A 49-year-old male presented to the emergency department with abdominal pain and generalized weakness. The physical examination was positive for right upper quadrant tenderness and positive Murphy’s sign. Point-of-care biliary ultrasound revealed signs of emphysematous cholecystitis. Emphysematous cholecystitis is a rare biliary pathology with a high mortality rate. It differs from acute cholecystitis is many ways. It has unique ultrasound characteristics. This case highlights the use of point-of-care ultrasound to diagnose a rare biliary condition.
CASE PRESENTATION
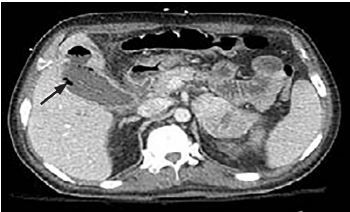
A 49-year-old man presented to the emergency department with epigastric abdominal pain. He was known to have multiple myeloma and was on chemotherapy; he also had a mass in the head of the pancreas, which required endoscopic retrograde cholangiopancreatography and stenting one month prior to this presentation. He was hypotensive and tachycardic. Abdominal exam revealed right upper quadrant tenderness and a positive Murphy’s sign. Point-of-care biliary ultrasound revealed gallstones, pericholecystic fluid, and punctate hyperechoic foci in the lumen of the gallbladder (Video). Computed tomography revealed a distended gallbladder with intraluminal gas extending into the inferior surface of the liver (Image). The patient underwent percutaneous cholecystostomy. The bile culture grew the gram-negative bacterium Prevotella buccae.
DISCUSSION
Emphysematous cholecystitis (EC) is diagnosed by the presence of gas in the lumen or the wall of the gallbladder in the setting of acute cholecystitis. It is a rare biliary pathology with a high mortality rate.1 EC differs from acute cholecystitis in many ways. It is more common in men and diabetics, and one third of the cases are not associated with cholethiasis.2 It is thought to be due to an ischemic event followed by an infection with gas-forming bacteria. The causative organism identified in this case is rare. The most common bacteria associated with this condition are Clostridium species, Escherichia coli, Klebsiella species, and anaerobic streptococci.1
The appearance of EC on ultrasound differs depending on the amount of gas in the gallbladder. A small amount of gas will produce echogenic foci with reverberation artifact known as ring-down artifact. However, a large amount of gas will produce a band with posterior dirty shadowing.3-4 Gas can also form multiple echogenic foci that move from the dependent to the independent area within the lumen of the gallbladder, also known as “effervescent gallbladder” or the “champagne” sign.4 Computed tomography is more sensitive and specific for the diagnosis of this condition.5 EC is a surgical emergency that is managed with intravenous antibiotics and cholecystectomy. Alternatively, percutaneous cholecystostomy is used in patients who are high risk for surgery.5
CPC-EM Capsule
What do we already know about this clinical entity?
Emergency physicians commonly perform biliary point-of-care ultrasound to identify gallstones and acute cholecystitis.
What is the major impact of the image(s)?
This case describes the use of point-of-care ultrasound to diagnose Emphysematous Cholecystitis (EC), highlighting the unique ultrasound characteristic of this condition.
How might this improve emergency medicine practice?
Using point-of-care ultrasound to diagnose EC (a rare condition with high mortality rate) could help accelerate the diagnosis and management.
Footnotes
Section Editor: Rick A. McPheeters, DO
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
Documented patient informed consent and/or Institutional Review Board approval has been obtained and filed for publication of this case report.
Address for Correspondence: Rasha Buhumaid, MBBS, Mohammed Bin Rashid University of Medicine and Health Sciences, College of Medicine, Building 14, Dubai Healthcare City, PO Box 505055, Dubai, United Arab Emirates. Email: Rasha.buhumaid@mbru.ac.ae. 4:107 – 108
Submission history: Revision received September 26, 2019; Submitted November 3, 2019; Accepted November 18, 2019
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Smith E, Dillman J, Elsayes K, et al. Cross-sectional imaging of acute and chronic gallbladder inflammatory disease. Am J Roentgenol. 2009;192(1):188-96.
2. Zippel D, Shapiro R, Goitein O, et al. Emphysematous cholecystitis: Don’t be lulled Into complacency. J Emerg Med. 2011;41(4):400-1.
3. Wexler B, Panebianco N. The effervescent gallbladder: an emergency medicine bedside ultrasound diagnosis of emphysematous cholecystitis. Cureus. 2017;9(7):e1520.
4. Safwan M, Penny S. Emphysematous cholecystitis. J Diagn Med Sonogr. 2016;32(3):131-7.
5. Huang H, Chuang C, Yang P. Abnormal gas in the gallbladder: emphysematous cholecystitis. J Emerg Med. 2013;45(2):254-5.
SUPPLEMENTARY MATERIAL
Point-of-care biliary ultrasound identifying gallstones (white arrow), pericholecystic fluid (red arrow), and gas in the gallbladder lumen (green arrow).