
{kind=link}
| Author | Affiliation |
|---|---|
| Johnny Fong, MD | University of Nevada, Las Vegas School of Medicine, University Medical Center of Southern Nevada, Department of Emergency Medicine, Las Vegas, Nevada |
| Tony Zitek, MD | University of Nevada, Las Vegas School of Medicine, University Medical Center of Southern Nevada, Department of Emergency Medicine, Las Vegas, Nevada; Kendall Regional Medical Center, Department of Emergency Medicine, Miami, Florida |
CASE PRESENTATION
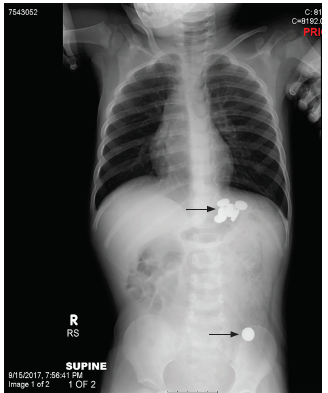
A two-year-old male presented to the pediatric emergency department for possible foreign body ingestion. Two hours prior to arrival, the child was found with the packaging for 10 button batteries, but his mother was only able to find one battery. The patient had no symptoms. Physical exam was within normal limits. Radiographs (Image 1) showed six foreign bodies within the stomach and one distally.
DISCUSSION
Button battery ingestions are increasing in both frequency as well as in major or fatal outcomes.1 A low threshold for imaging is important as 54% of fatalities are from misdiagnosis due to non-specific presentations.1 Possible complications include perforations, fistula, strictures, hemorrhage, and death.2 The National Capital Poison Center Button Battery Ingestion Triage and Treatment Guideline (National Button Battery Guideline) specifically addresses patient age, battery size and location, and symptoms; however; it does not specifically address ingestion of multiple button batteries.3
The National Button Battery Guideline was recently changed to include the immediate administration of oral honey. This update was based on a recent study showing both in vitro and in vivo protective effects of honey in button battery ingestion.4 Imaging is not required if a specific set of criteria are met; otherwise, radiographs should be obtained of the entire length of the gastrointestinal tract to locate the battery.3 The main considerations are whether the battery is in the esophagus, if a magnet was co-ingested, or if the patient is having any symptoms.3 In these cases, endoscopic removal is preferred; however, surgical removal may be necessary if the battery is beyond reach.3 Important consideration should also be given to delayed injuries after battery removal.3
CPC-EM Capsule
What do we already know about this clinical entity?
The National Button Battery Guideline does not offer specific recommendations for multiple battery ingestions, an entity which is not well discussed in the existing literature.
What is the major impact of the image(s)?
Through providing initial and subsequent radiographs, this case aims to increase awareness of button battery ingestions, which is increasing in both frequency and major outcomes.
How might this improve emergency medicine practice?
This case offers a successful example of diagnosis and management of a multiple button battery ingestion through admission for whole-bowel irrigation with polyethylene glycol.
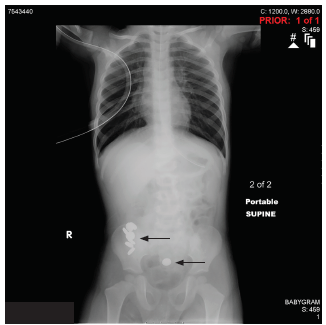
This patient was admitted for observation, serial abdominal exams, and polyethylene glycol whole-bowel irrigation. Radiograph the next morning showed progression of the batteries (Image 2). Whole-bowel irrigation continued and eventually nine button batteries were passed rectally. Follow-up radiographs did not show any retained batteries.
Footnotes
Section Editor: Steven Walsh, MD
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
Documented patient informed consent and/or Institutional Review Board approval has been obtained and filed for publication of this case report.
Address for Correspondence: Johnny Fong, MD, University of Nevada, Las Vegas School of Medicine, University Medical Center of Southern Nevada, Department of Emergency Medicine, 5298 Caprock Canyon Ave, Las Vegas, NV 89139. Email: johnny.fong.em@gmail.com. 3:156 – 157
Submission history: Revision received July 1, 2018; Submitted October 21, 2018; Accepted November 7, 2018
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Litovitz T, Whitaker N, Clark L, et al. Emerging battery-ingestion hazard: clinical implications. Pediatrics. 2010;125(6):1168-77.
2. Injuries from batteries among children aged <13 years–United States, 1995–2010. MMWR Morb Mortal Wkly Rep. 2012;61(34):661-6.
3. National Capital Poison Center Button Battery Ingestion Triage and Treatment Guidelines. 2016. Available at: https://www.poison.org/battery/guideline. Accessed October 21, 2018.
4. Anfang RR, Jatana KR, Linn RL, et al. pH-neutralizing esophageal irrigations as a novel mitigation strategy for button battery injury. Laryngoscope. 2019;129(1):49-57.