
{kind=link}
| Author | Affiliation |
|---|---|
| Arielle E. Schwitkis, BA | Cedars-Sinai Medical Center, Department of Emergency Medicine, Los Angeles, California |
| Talia L. Pollack, PA-C | Cedars-Sinai Medical Center, Department of Emergency Medicine, Los Angeles, California |
| Sam S. Torbati, MD | Cedars-Sinai Medical Center, Department of Emergency Medicine, Los Angeles, California |
CASE PRESENTATION
An 80-year-old woman with a history of hypertension presented to the emergency department (ED) with blunt facial trauma including a four-centimeter laceration of the right upper eyelid sustained during a ground-level mechanical fall. Upon arrival to the ED, she was confused, repetitive, and amnesic to events surrounding the fall. Computed tomography (CT) of the brain and orbits was rapidly obtained, and upon return from CT she reported new visual loss of the right eye with the ability to see only light. On exam, her globe was noted to be increasingly firm, full to palpation, and swollen shut. Physical examination also revealed new ophthalmoplegia, proptosis, subconjunctival hemorrhage, and afferent pupillary defect. Intraocular pressure (IOP) measured 50 mmHg in the right eye and 12 mm Hg in the left eye. CT demonstrated a hematoma within the right orbit impinging on orbital contents, confirming the diagnosis of orbital compartment syndrome (OCS). An emergent bedside lateral canthotomy and cantholysis (LCC) was performed by the emergency physician with reduction of her IOP and restoration of vision.
DISCUSSION
OCS is a rare complication of increased pressure within the confined orbital space. It may be caused by retro-orbital hematoma following blunt or penetrating trauma to the orbit. The pressure exerted by the hematoma reduces perfusion resulting in ischemia-induced vision loss, which may develop over minutes to hours.1-3 OCS may present with ocular pain, diplopia, or vision loss.4,5 OCS is a clinical diagnosis with physical examination findings that may include ophthalmoplegia, proptosis, subconjunctival hemorrhage, and afferent pupillary defect.1,4,5 Diagnostic criteria include a constellation of the aforementioned signs and symptoms associated with an IOP of 30 mmHg or higher.2,6 LCC, the primary treatment for OCS, is a relatively simple procedure ideally performed within 60–120 minutes of symptom onset to prevent permanent vision loss.1,3,4,7
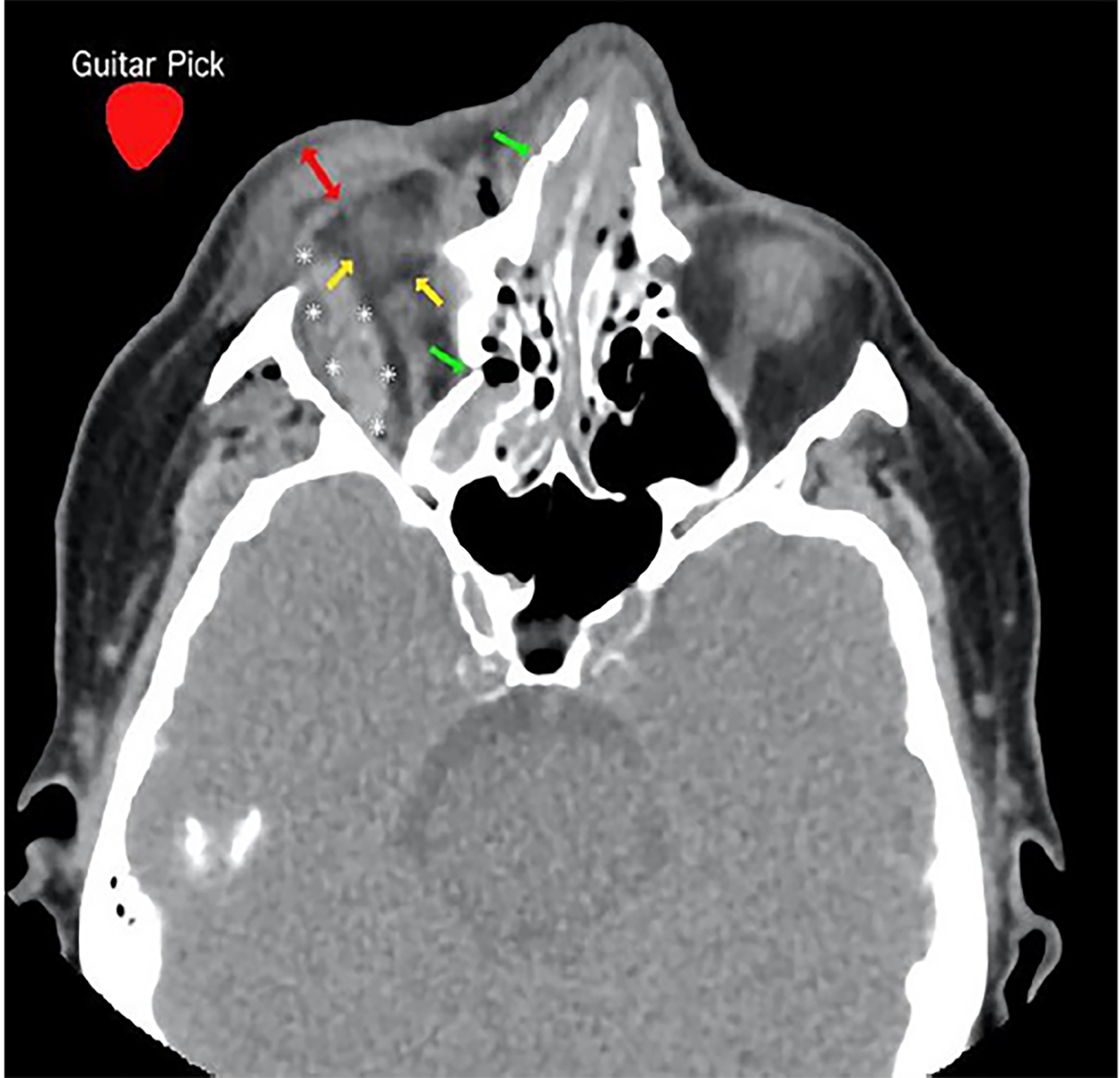
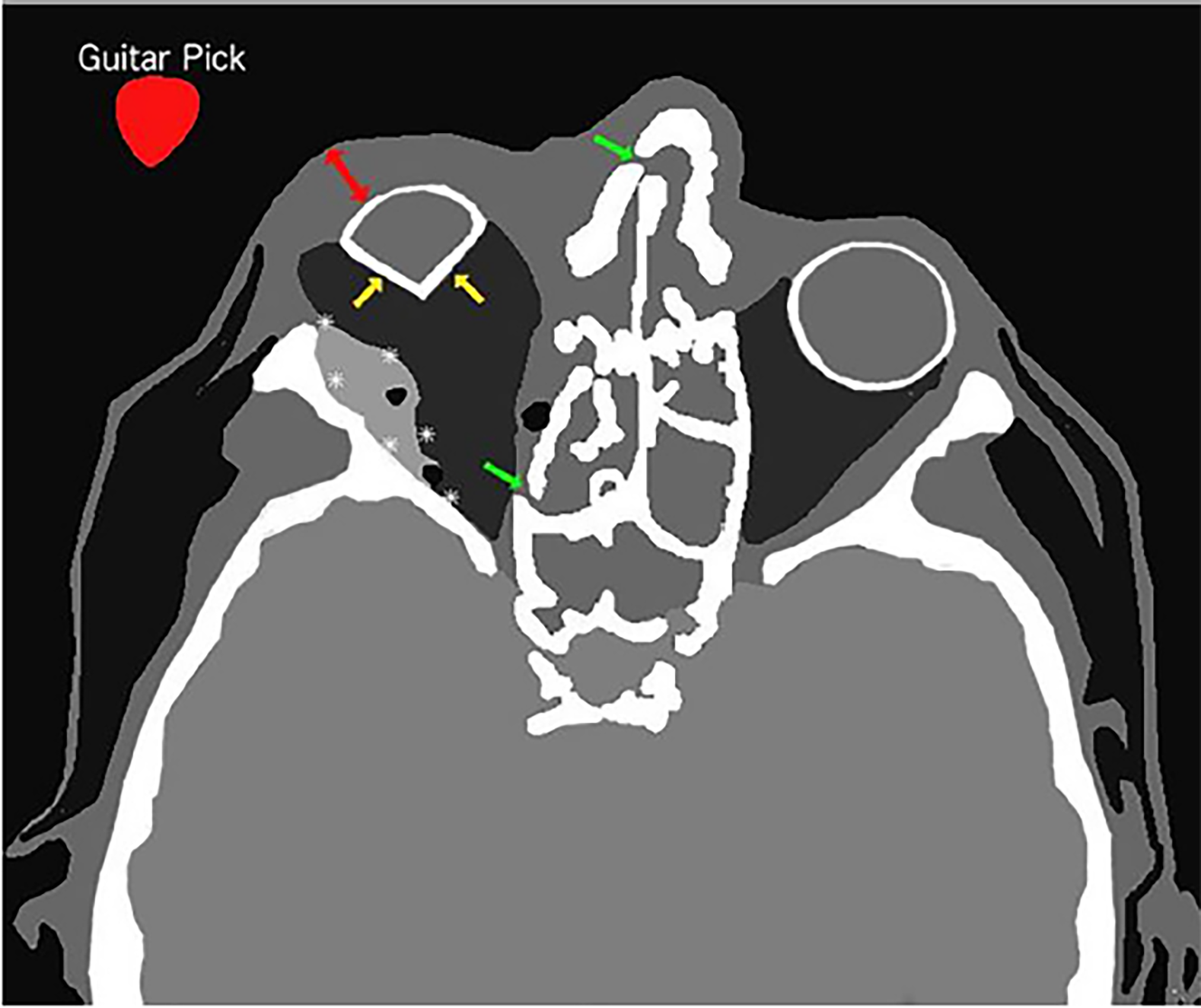
Diagnosis of OCS can be challenging as the patient’s examination may be limited by altered mental status; vision loss may be masked by inability to open edematous eyelids; and orbital pain may be explained by bony and soft tissue injury.7 CT findings concerning for OCS include tenting of the posterior sclera – otherwise known as “guitar pick” sign – caused by intraocular mass (Images 1 and 2).8 Although CT findings of retro-orbital hematoma should raise suspicion for OCS, serial evaluations are essential for detecting OCS in evolution.
Documented patient informed consent and/or Institutional Review Board approval has been obtained and filed for publication of this case report.
CPC-EM Capsule
What do we already know about this clinical entity?
Orbital compartment syndrome is a rare complication of increased pressure within the confined orbital space that may lead to permanent blindness if not treated in a timely fashion.
What is the major impact of the image(s)?
The “guitar pick” sign is a rarely reported radiographic sign that should alert physicians of the possibility of a syndrome requiring immediate intervention.
How might this improve emergency medicine practice?
Emergency physicians will be able to better recognize patients at risk for orbital compartment syndrome following blunt facial trauma.
Footnotes
Section Editor: Shadi Lahham, MD
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
Address for Correspondence: Arielle E. Schwitkis, BA, Cedars-Sinai Medical Center, Department of Emergency Medicine, 8700 Beverly Blvd., Los Angeles, CA 90048. Email: Arielle.Schwitkis@cshs.org. 2:268 – 269
Submission history: Revision received January 30, 2018; Submitted April 19, 2018; Accepted April 25, 2018
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Rowh AD, Ufberg JW, Chan TC, et al. Lateral canthotomy and cantholysis: emergency management of orbital compartment syndrome. J Emerg Med. 2015;48(3):325-30.
2. Sun MT, Chan OW, Selva D. Traumatic orbital compartment syndrome: importance of lateral canthomy and cantholysis. Emerg Med Australas. 2014;26(3):274-8.
3. Ujam A, Perry M. Emergency Management for orbital compartment syndrome—is decompression mandatory?. Int J Oral Maxillofac Surg. 2016;45(11):1435-7.
4. Fontenot TE, Carter JM, Friedlander P. Eye pain after traumatic orbital fracture. JAMA Otolaryngol Head Neck Surg. 2014;140(9):877-8.
5. Scott M, Thomson A. Prompt Recognition and treatment in traumatic retro-orbital hematoma in anticoagulated elderly people can save sight. J Am Geriatr Soc. 2009;57(3):568-9.
6. Capek KD, Culnan DM, Merkley K, et al. Burn Injuries of the Eye. Total Burn Care. 2018:435-4.e6.
7. Kniess CK, Fond TC, Reilly AJ, et al. Early detection of traumatic retrobulbar hemorrhage using bedside ocular ultrasound. J Emerg Med. 2015;49(1):58-60.
8. Minkis K, Whittington A, Alam M. Dermatologic surgery emergencies. J Am Acad Dermatol. 2016;75(2):265-284.