
{kind=link}
| Author | Affiliation |
|---|---|
| Halsey Jakle, MD | Kern Medical, Department of Emergency Medicine, Bakersfield, California |
| Adria Winter, MD | Kern Medical, Department of Emergency Medicine, Bakersfield, California |
| Natalie Pena, BS | Kern Medical, Department of Emergency Medicine, Bakersfield, California |
INTRODUCTION
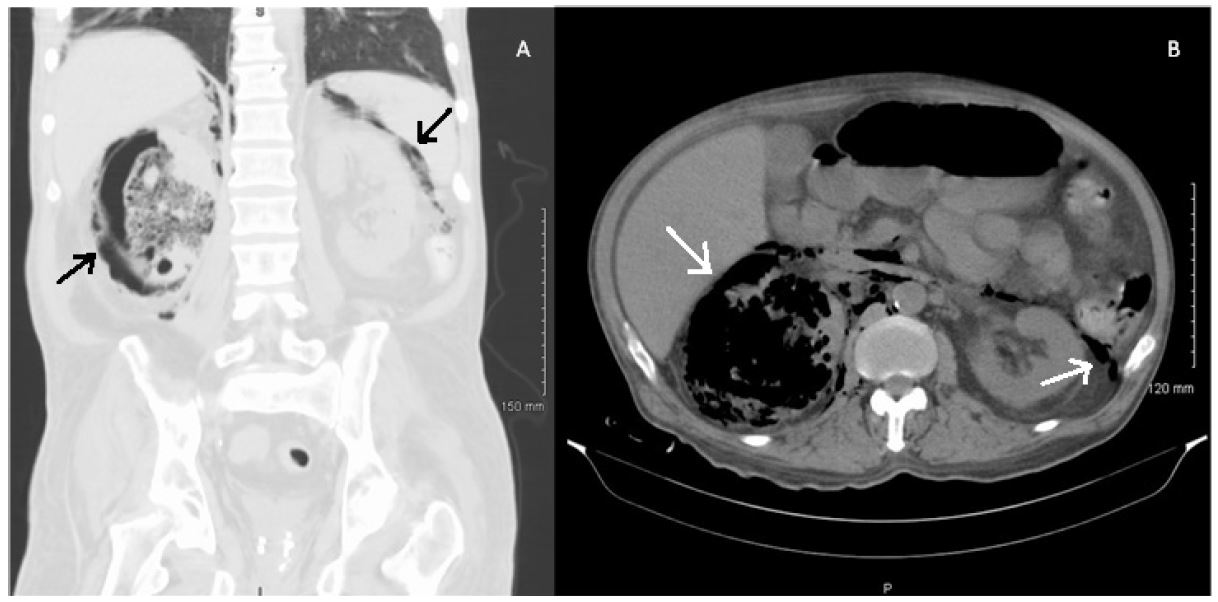
A 58-year-old male presented to an outside hospital with altered mental status and right flank pain for three days. Septic work up, including computed tomography of the abdomen and pelvis, were significant for diabetic ketoacidosis, pyelonephritis, and significant air replacing much of the right kidney, consistent with emphysematous pyelonephritis (Image). The patient was transferred to our facility for a higher level of care.
The patient was stabilized, given intravenous (IV) antibiotics, and admitted to the intensive care unit with a diagnosis of septic shock secondary to emphysematous pyelonephritis.
DISCUSSION
Our case presents an image of a condition that is rare and particularly severe, as shown by free air not only in the right renal parenchyma, but also extending outside the capsule, around the renal vasculature, and into the left peri-renal space.
Emphysematous pyelonephritis is a relatively rare infection, seen only 1–2 times per year in a typical busy urological department in the United States. It affects patients with diabetes in 95% of cases. E. coli and Klebsiella account for over 90% of cases, although Proteus mirabilis, Pseudomonas, and Streptococcus are also seen. Gas accumulates due to rapid necrosis of the renal parenchyma and peri-renal tissue, as opposed to gas appearing as a byproduct of anaerobic bacteria as is the case in necrotizing fasciitis. The condition is fatal if not treated appropriately, and the mainstay of treatment is nephrectomy in conjunction with IV antibiotics for severe, disseminated infection.
Footnotes
Section Editor: Rick A. McPheeters, DO
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
Address for Correspondence: Halsey Jakle, MD, Kern Medical Emergency Department, 1700 Mount Vernon Ave, Bakersfield, CA 93306. Email: hjakle@gmail.com. 1:61 – 62
Submission history: Revision received October 11, 2016; Accepted November 8, 2016
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. May T, Stein A, Molnar R, et al. Demonstrative Imaging of Emphysematous Cystitis. Urol Case Rep. 2016(6):56-7.
2. Ouellet LM, Brook MP. Emphysematous Pyelonephritis: An Emergency Indication for the Plain Abdominal Radiograph. Ann Emerg Med. 1988;17(7):722-4.
3. Huang J, Tseng C. Emphysematous pyelonephritis: clinicoradiological classification, management, prognosis, and pathogenesis. Arch Intern Med. 2000;160:797-805.