
{kind=link}
| Author | Affiliation |
|---|---|
| Kiran K. Gudivada, MD | St. John’s Medical College Hospital, Department of Critical Care Medicine, Bangalore, Karnataka, India |
CASE PRESENTATION
We present two cases of cerebrovascular accidents. Case #1: A 24-year-old man presented with open fractures of the left femur and tibia after a motor vehicle collision. Within two hours, he developed left facio-bracial paresis. Although he arrived in the window period for thrombolysis, polytrauma precluded thrombolysis. His modified Rankin Scale (mRS) score at admission was five. Case #2: A 26-year-old man presented to the emergency department after eight hours with hemiplegia and global aphasia. His admission mRS score was four. Stroke workuprevealed hyperhomocysteinemia (>114 μmol/L).
DIAGNOSIS
In Case #1, considering the background of trauma and imaging suggestive of luminal filling defect, we suspected an internal carotid artery (ICA) dissection.1 The proposed mechanism was the hyperextension of the neck due to decelerating forces during trauma, causing stretch of ICA over the cervical vertebrae. This resulted in shear stress and intimal tear, acting as a nidus for the thrombus formation.2 In Case #2, hyperhomocysteinemia is the risk factor for thrombus formation leading to stroke. After four weeks, there was a complete resolution of thrombus and the mRS score improved to two in Case #2 with oral antiplatelet and anticoagulation therapy, while Case #1 was lost to follow-up. In both cases, family refused to consent for mechanical thrombectomy.
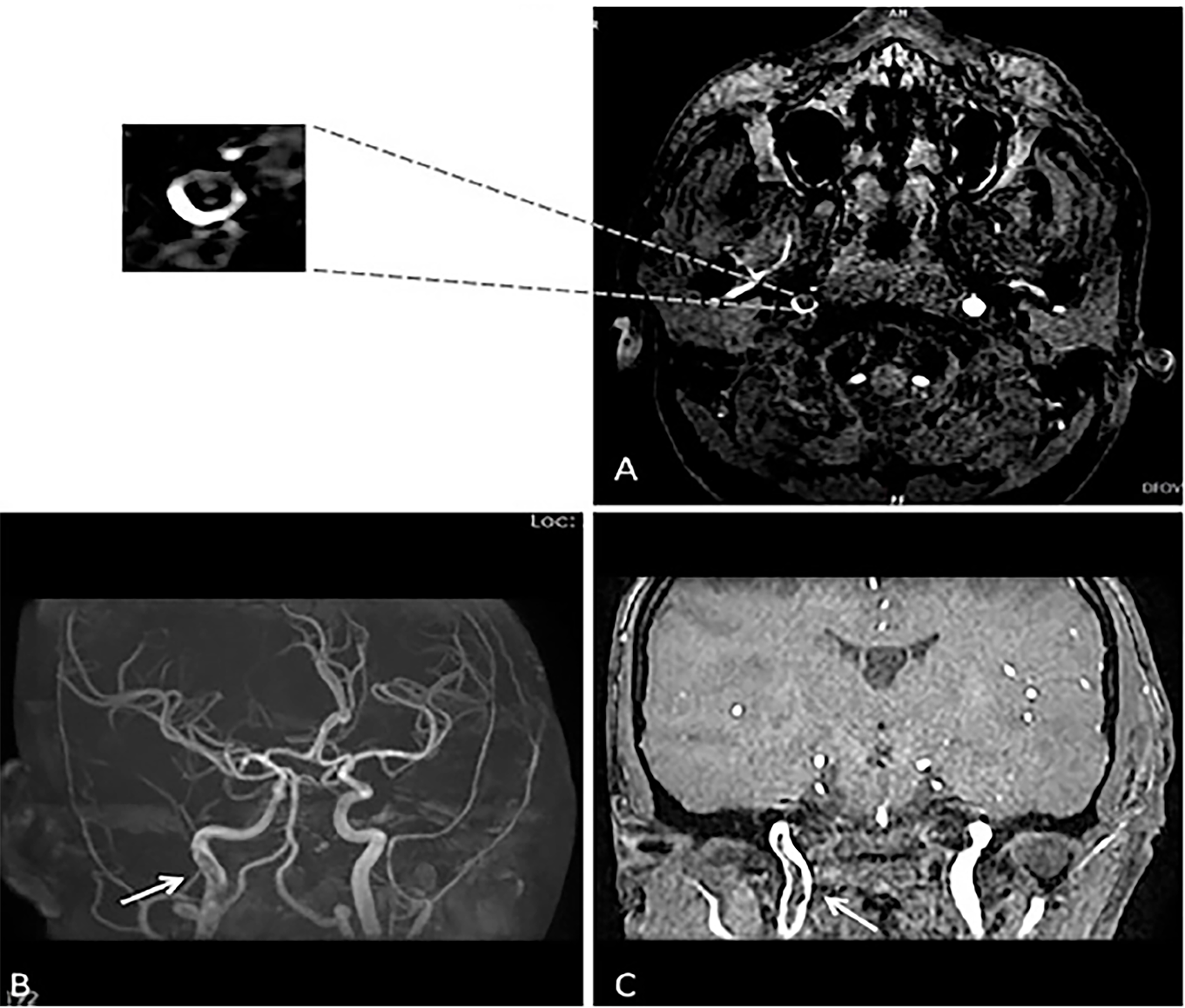
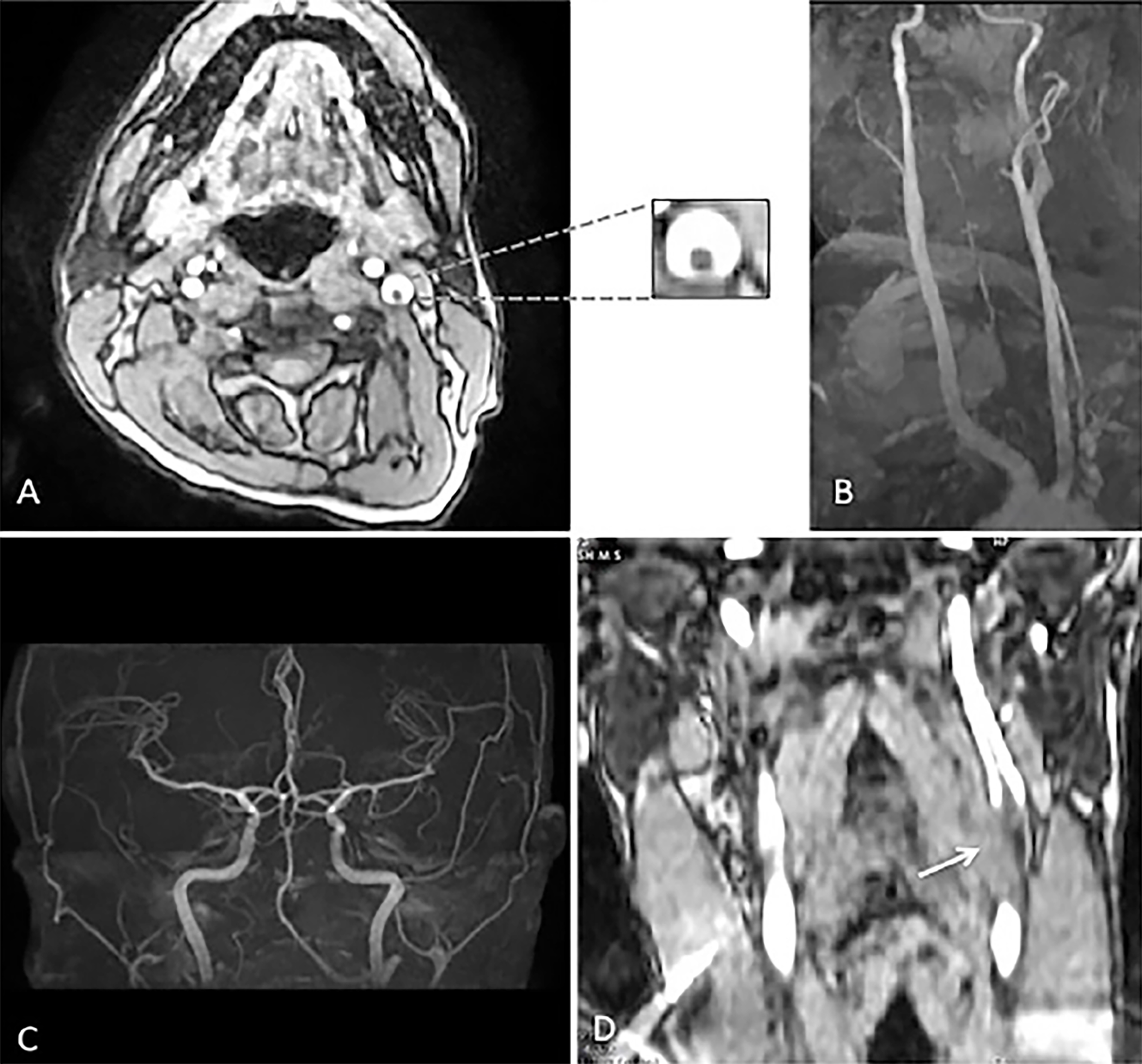
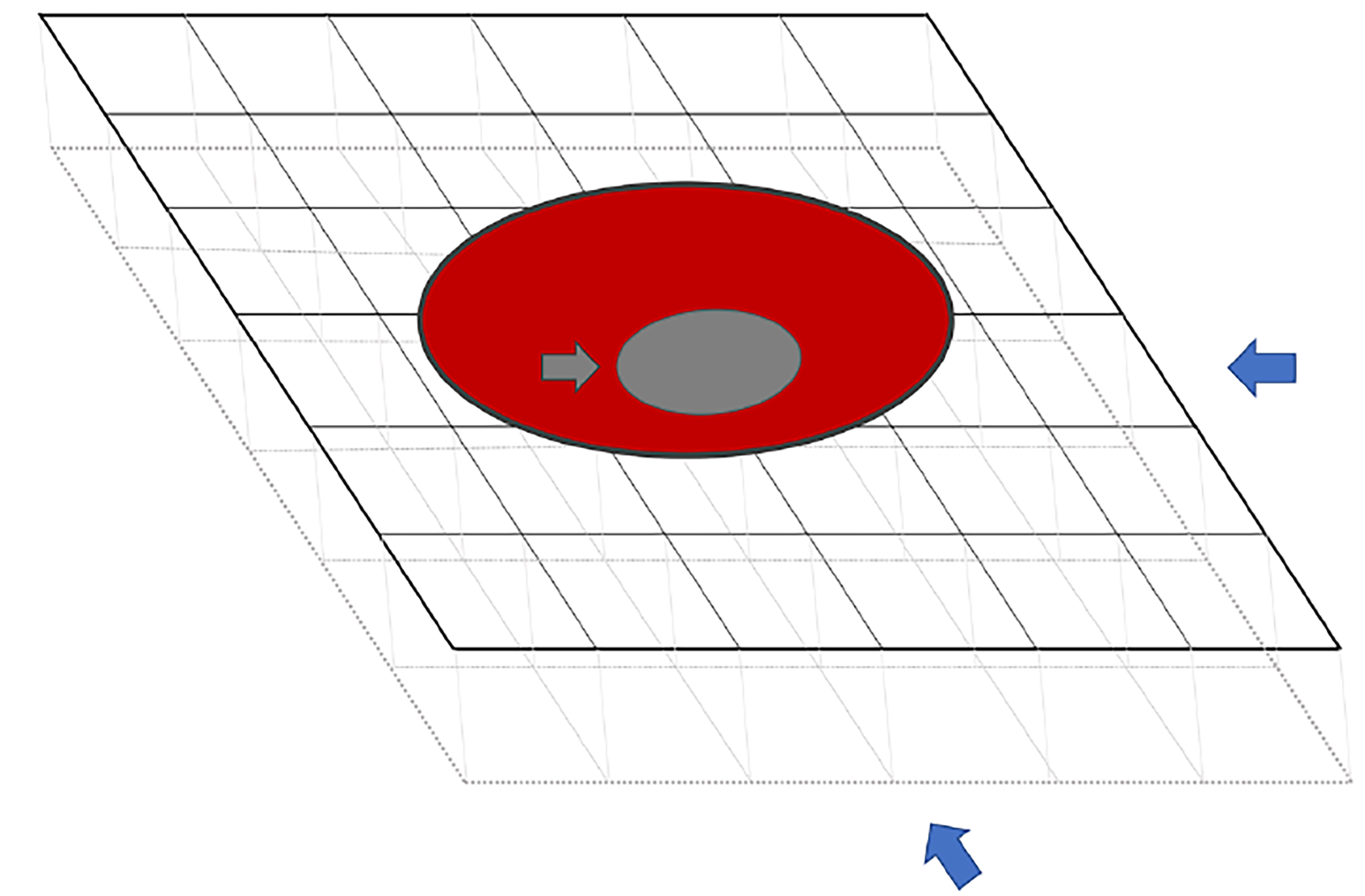
In the literature, luminal thrombus in the ICA has been described radiologically with various analogies such as “donut sign,” “crescent sign,” or “string sign.”3 Although these radiological signs guide us to localize the lesion, they should be interpreted with caution. In Case #1, maximum intensity projection (MIP) image of magnetic resonance angiography (MRA) head showed a filling defect in the right ICA (Image 1B), while in Case #2 there was no definitive filling defect seen in MRA-MIP of the left ICA (Images 2B and 2C). However, thrombus was identified in the axial source images of the neck in both cases (Images 1A and 2A). The probable explanation for the false negative MIP images in Case #2 could be the flow-related alteration in image enhancement. For instance, intraluminal thrombus may become inapparent if surrounded by hyperintense blood flow and a falsely normal-appearing blood vessel can be reconstructed (Image 3).4 Therefore, it is always advisable to refer to the individual source images while interpreting the MIP image.4
In summary, these images emphasize two practical points: 1) limitations in the interpretation of MRA-MIP image (false negatives); and 2) the significance of evaluating source images of head and neck in stroke workup.
CPC-EM Capsule
What do we already know about this clinical entity?
Cerebrovascular accidents are the most common neurological emergencies. Magnetic resonance imaging (MRI) and MR angiography are the recommended modalities to identify stroke etiology.
What is the major impact of the image(s)?
These radiological images highlight the major limitation of maximum intensity projection images in detecting the intraluminal thrombus.
How might this improve emergency medicine practice?
Knowledge of basic MRI interpretation and its limitation will aid the emergency physician in prompt diagnosis, etiological differentiation and subsequent management of stroke.
Documented patient informed consent and/or Institutional Review Board approval has been obtained and filed for publication of this case report.
Footnotes
Section Editor: Shadi Lahham, MD, MS
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
Address for Correspondence: Kiran K. Gudivada, MD, Department of Critical Care Medicine, Silver Jubilee Block, St. John’s Medical College Hospital, Sarjapur Main Road, Bangalore 560034, Karnataka, India Bangalore 560034, Karnataka, India. Email: gkiran17medico@gmail.com. 2:365 – 366
Submission history: Revision received May 23, 2018; Submitted June 24, 2018; Accepted July 5, 2018
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Haneline MT, Rosner AL. The etiology of cervical artery dissection. J Chiropr Med. 2007;6(3):110-20.
2. Fabian TC, Patton JH, Croce MA, et al. Blunt carotid injury. Importance of early diagnosis and anticoagulant therapy. Ann Surg. 1996;223(5):513-25.
3. Menon BK, Singh J, Al-Khataami A, et al. The donut sign on CT angiography: an indicator of reversible intraluminal carotid thrombus?. Neuroradiology. 2010;52(11):1055-6.
4. Tsuruda J, Saloner D, Norman D. Artifacts associated with MR neuroangiography. Am J Neuroradiol. 1992;13(5):1411-22.